Youth's Lives Every Day
About the Trevor Project
The Trevor Project is the world’s largest suicide prevention and crisis intervention organization for lesbian, gay, bisexual, transgender, queer & questioning (LGBTQ) young people. The Trevor Project offers a suite of 24/7 crisis intervention and suicide prevention programs, including TrevorLifeline, TrevorText, and TrevorChat as well as the world’s largest safe space social networking site for LGBTQ youth, TrevorSpace. Trevor also operates an education program with resources for youth-serving adults and organizations, an advocacy department fighting for pro-LGBTQ legislation and against anti-LGBTQ rhetoric/policy positions, and a research team to discover the most effective means to help young LGBTQ people in crisis and end suicide. If you or someone you know is feeling hopeless or suicidal, our trained crisis counselors are available 24/7 at 1-866-488-7386 via chat www.TheTrevorProject.org/Help, or by texting START to 678-678.
About This Work
Significant increases in suicide deaths have occurred over the past 10 years in the U.S., particularly among adolescents and young adults (Curtin & Heron, 2019). However, suicide can be prevented through comprehensive public health strategies aimed at reducing risk factors and increasing protective factors (The Trevor Project, 2019a). Increased knowledge about populations at highest risk for suicide can assist prevention efforts aimed at ending suicide and enhancing well-being for those individuals. National prevalence data on lesbian, gay, and bisexual (LGB) high school students, collected as part of the Centers for Disease Control and Prevention’s (CDC) Youth Risk Behavior Surveillance System (YRBS), indicate that LGB youth are more than four times as likely to attempt suicide compared to straight peers (Kann et al., 2018). Recently, the CDC released a report focused on transgender high school students, with similar disparities found in suicidality among transgender compared to cisgender students as between LGB and straight students (Johns et al., 2019). Further, The Trevor Project’s 2019 National Survey on LGBTQ Youth Mental Health found that 39% of LGBTQ youth ages 13–24 reported seriously considering suicide in the previous 12 months (The Trevor Project, 2019b). Among adults, individuals ages 18–25 have the highest rates of suicide attempts (Substance Abuse and Mental Health Services Administration, 2019). Thus, there is an urgent need to understand suicide disparities among LGB young adults ages 18–25, including how they compare to findings among high school students. In 2015 the Substance Abuse and Mental Health Services Administration’s (SAMHSA) National Survey on Drug Use and Health (NSDUH) included questions on sexual identity for the first time. The NSDUH is currently the only national-level dataset to use probabilistic sampling and include questions on both sexual identity and suicidality among this age group. This report is the first to compare findings on suicidality among LGB youth ages 18–25 to those among LGB U.S. high school students, including the provision of adjusted odds ratios to assess suicidality risk among LGB youth compared to straight peers.
Key Findings
The magnitude of disparities in suicidality between straight and LGB adolescents persists into young adulthood.
- Even when adjusting for additional factors, LGB young adults ages 18–25 were more than four times as likely to report planning and attempting suicide in the past year compared to straight peers.
- 10.4% of LGB youth ages 18–25 reported making a suicide plan in the past year compared to 2.6% of straight peers.
- 5.7% of LGB youth ages 18–25 reported a suicide attempt in the past year compared to 1.3% of straight peers.
LGB young adults ages 18–25 were three times as likely to report a major depressive episode in the past year compared to their straight peers.
- 30.9% of LGB youth ages 18–25 met criteria for a major depressive episode in the past year compared to 11.1% of straight peers.
- A greater proportion of bisexual young adults ages 18–25 met criteria for a major depressive episode (32.7%) compared to gay/lesbian young adults (26.8%).
The data currently collected do not allow for nationally representative analyses on gender identity or suicide deaths.
- National surveys of youth and young adult experiences now include questions on sexual identity but do not consistently include questions on gender identity.
- Death record databases do not currently include accurate information on sexual identity and gender identity that would allow for analyses to include deaths by suicide in addition to suicide ideation and attempts.
Methodology Summary
Prevalence rates by sexual identity for past year suicidal thoughts, plans, and attempts are compared to rates among high school students based on the 2017 YRBS. NSDUH diagnostic prevalence rates are provided for major depressive disorder based on the Diagnostic and Statistical Manual of Mental Disorders criteria. Logistic regressions were used to predict suicidality among youth ages 18–25 based on sexual identity while controlling for sex, race/ethnicity, and income. For high school students, logistic regressions were conducted to predict depressive symptoms and suicidality while adjusted for race/ethnicity and gender.
Notes on Terminology
The acronym LGB is used rather than LGBTQ, as the NSDUH dataset does not collect data on transgender, queer, or questioning identities. Additionally, we focus on ages 18–25 rather than 18–24, as the most detailed age variable in the 2018 NSDUH dataset combines ages 24 and 25 rather than providing discrete single ages. YRBS data are representative of high school students in the U.S., with the majority of students (87%) falling between the ages of 14 and 17.
BACKGROUND
Significant increases in suicide deaths have occurred over the past 10 years in the U.S. (Curtin & Heron, 2019). Suicide is the second leading cause of death among individuals ages 10–24 (Hedegaard, Curtin, & Warner, 2018), and previous suicide attempts are one of the strongest predictors of death by suicide (Dervi, Brent, & Oquendo, 2008). Further, in a recent global meta-analysis, those diagnosed with depression were at nine times greater risk of dying by suicide (Conner et al., 2019). Suicide can be prevented through comprehensive public health strategies aimed at reducing risk factors and increasing protective factors (The Trevor Project, 2019a). Increased knowledge about populations at highest risk for suicide can assist prevention efforts aimed at ending suicide and enhancing well-being for those individuals. Lesbian, gay, bisexual, transgender, queer, or questioning (LGBTQ) individuals are particularly vulnerable due to heightened minority stress, marked by increased victimization, rejection, and the internalization of LGBTQ stigma (Meyer, 2003).
Research on LGBTQ populations has been slowed by a lack of federally collected data on sexual identity and gender identity. Despite decades of research indicating that LGBTQ individuals are exposed to minority stress, which increases risk for experiencing challenges related to depression and suicidality (Meyer, 2003), national-level prevalence studies have only recently begun to include items on sexual identity and gender identity. In 2015 the Centers for Disease Control and Prevention’s (CDC) Youth Risk Behavior Surveillance System (YRBS) included a question to ascertain sexual identity for the first time in its standard questionnaire used by the states and large urban school districts. There data were crucial for documenting adverse mental health indicators among lesbian, gay, and bisexual (LGB) high school students, including greater depressive symptoms and more than four times the rate of attempting suicide in the past 12 months compared to straight peers. In 2017, 10 states and nine large urban school districts included a YRBS question to measure the proportion of high school students who identify as transgender. Analysis of this dataset revealed that a higher proportion of transgender students reported all suicide risk outcomes, including seriously considering, planning, and attempting suicide, compared to cisgender students. YRBS findings have been prominently featured by the CDC in published reports on sexual identity and gender identity (Kann et al., 2016; Johns et al., 2018; Johns et al., 2019). The widespread dissemination of YRBS findings on suicidality can support policies, programs, and practices aimed at reducing disparities for LGBTQ high school students.
Representative data on LGBTQ young adults over the age of 18 has not been widely disseminated or compared to disparities among high school students. In 2015, the National Survey on Drug Use and Health (NSDUH) added a question on sexual identity. The NSDUH is administered annually and is the only nationally representative source of federally collected information on suicidality among LGB adults. Given that the highest rates of suicide attempts among adults occur among those ages 18–25 (Substance Abuse and Mental Health Services Administration, 2019), and findings that LGB high schools students are more than four times as likely to attempt suicide compared to straight peers (Kann et al., 2016), there is a dire need for widely disseminated findings related to suicidality among LGB young adults ages 18–25. A clear understanding of disparities in depression and suicidality by sexual identity among not only high school aged youth, but also those ages 18–25, is necessary to inform national prevention strategies, advocate for policy changes, and advance research efforts.
METHODOLOGY
NSDUH and YRBS Comparative Analyses. All NSDUH analyses were conducted for young adults ages 18 to 25 years using the most recent dataset collected in 2018. All YRBS analyses were conducted for high school aged youth using the most recent dataset collected in 2017. Descriptive analyses were conducted with both NSDUH and YRBS data by sexual identity (gay/lesbian, bisexual, and straight) to estimate the proportion of individuals who identify as LGB as well as the 12-month prevalence of suicidal ideation (seriously think about trying to kill themselves in the past 12 months), suicide plan (making a plan to kill themselves in the past 12 months), and suicide attempt (attempting suicide one or more times in the past 12 months). For youth ages 18–25, estimates by sexual identity are provided for past year major depressive episode using Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria, as collected in the 2018 NSDUH. Although the YRBS does not collect diagnostic data to determine criteria for a major depressive episode, it does include a single item asking youth whether they felt so sad or hopeless nearly every day for at least two weeks in the past year that they stopped doing some usual activities. We provide this data for illustrative purposes of examining disparities related to symptoms of depression; however, the two measures are conceptually distinct and should not be directly compared.
NSDUH and YRBS use a complex, multistage sampling strategy and provide sampling weights to generate estimates of the U.S. civilian, noninstitutionalized population and U.S. high school students, respectively. For all analyses, the complex samples module of SPSS 25 was used to account for the complex sample design and sample weights for the NSDUH and YRBS datasets.
Adjusted Odds of Suicidality and Depression. Multivariate logistic regression models were applied to examine the association of sexual identity (LGB compared to straight) with suicidality (seriously considering suicide, making a suicide plan, and suicide attempts), and major depressive episode) among young adults ages 18–25 after controlling for race/ethnicity, gender, and federal poverty status. Because the YRBS does not include an indicator of socioeconomic status, logistic regressions were conducted to predict depressive symptoms and suicidality while adjusted for race/ethnicity and gender.
RESULTS
Comparing High School Students to Youth Ages 18–25
Sexual identity. Nearly 12% of young adults ages 18–25 identified as gay/lesbian (2.8%) or bisexual (8.9%). Prevalence rates for gay/lesbian (2.4%) and bisexual (8.0%) high school students in the 2017 YRBS were not significantly different from those obtained for those ages 18–25. The percentage of individuals who were unsure of their sexual identity was significantly less among those ages 18–25 with less than one percent (.6%) indicated that they did not know their sexual identity, compared to 4.2% among high school students who indicated they were “not sure.”
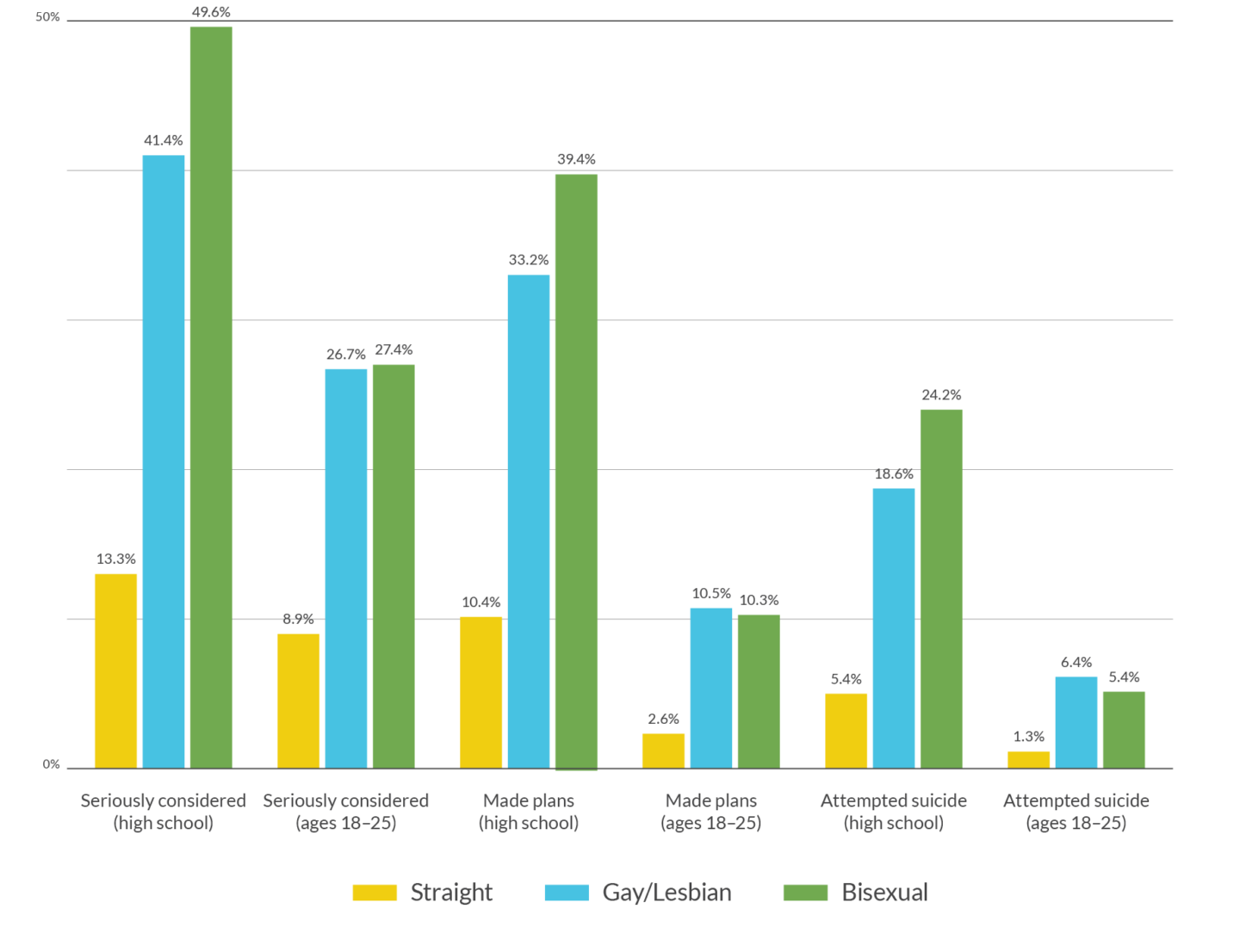
Suicidality. A significantly higher proportion of LGB high school students and young adults ages 18–25 reported seriously considering, planning, and attempting suicide compared to straight peers (See Table 1). Overall, rates of seriously considering, planning, and attempting suicide were significantly lower among youth ages 18–25 compared to high school students. The magnitude of the disparities between straight and LGB youth for seriously considering suicide in the past year were reduced among those ages 18–25 (8.9% straight vs. 27.3% LGB) compared to high school students (13.3% straight vs. 47.7% LGB). However, the magnitude of disparities for making a plan to attempt suicide among those ages 18–25 (2.6% straight vs. 10.4% LGB) compared to high school students (10.4% straight vs. 38.8% LGB) and attempting suicide among those ages 18–25 (1.3% straight vs. 5.7% LGB) compared to high school students (23.0% straight vs. 38.8% LGB) remained relatively stable. Figure 1 provides prevalence rates for lesbian/gay, bisexual, and straight youth for each suicidality indicator among high school students based on YRBS data and among young adults ages 18–25 based on NSDUH data. A larger percentage of bisexual high school students endorsed each suicidality indicator compared to gay/lesbian students, with the proportion of bisexual and gay/lesbian youth ages 18–25 who reported suicidality being virtually identical.
Table 1. Weighted Prevalence Rates of Past Year Suicidality by Sexual Identity
| High School Students Straight | High School Students Lesbian/Gay/Bisexual | Ages 18–25 Straight | Ages 18–25 Lesbian/Gay/Bisexual | |||||
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | |
| Seriously thought about killing self in past year | 13.30% | 12.5–14.3% | 47.70% | 43.7–51.8% | 8.90% | 8.2–9.5% | 27.30% | 24.5–30.4% |
| Made plans to kill self in past year | 10.40% | 9.3–11.7% | 38.00% | 34.5–41.7% | 2.60% | 2.3–2.9% | 10.40% | 8.4–12.8% |
| Attempted to kill self in past year | 5.40% | 4.6–6.4% | 23.00% | 18.6–28.0% | 1.30% | 1.1–1.7% | 5.70% | 4.3–7.5% |
Figure 1: Weighted Prevalence Rates of Past Year Suicidality by Sexual Identity
Depression. Among LGB young adults ages 18–25, 30.9% met DSM criteria for a major depressive episode in the past year compared to 11.1% of straight peers. A greater proportion of bisexual young adults ages 18–25 met criteria for a major depressive episode (32.7%) compared to gay/lesbian young adults (26.8%). The YRBS uses a single item asking students whether they felt so sad or hopeless nearly every day for at least two weeks in the past year that they stopped doing some usual activities. Among LGB high school students, 63.0% endorsed this item on depressive symptoms, compared to 27.5% among straight high school students. Rates were higher for bisexual students (66.0%) compared to gay/lesbian students (53.1%).
Adjusted Odds of Depression and Suicidality
After controlling for race/ethnicity, gender, and poverty status, LGB individuals ages 18–25 were more than four times as likely to make a plan to attempt suicide (aOR=4.09, p<.001) and attempt suicide (aOR=4.27, p<.001), more than three and a half times as likely to seriously consider suicide (aOR=3.60, p<.001), and more than three times as likely to report a major depressive episode (aOR=3.20, p<.001) in the past year compared to their straight peers (See Table 2). After controlling for race/ethinicty and gender, LGB high school students were more than four and a half times as likely to make a plan to attempt suicide (aOR=4.78, p<.001) and more than four times as likely to attempt suicide (aOR=4.42, p<.001) compared to their straight peers. The 95% confidence intervals for making a suicide plan and attempting suicide overlap, indicating that any differences between the adjusted odds for high school students and those ages 18–25 are not significant. The adjusted odds of seriously considering suicide were higher among LGB high school students than among those ages 18–25, with LGB high school students (aOR=5.26, p<.001) more than five times as likely to seriously consider suicide as straight students. LGB high school students (aOR=3.76, p<.001) were almost four times more likely than straight high schools students to report feeling so sad or hopeless nearly every day for at least two weeks in the past year that they stopped doing some usual activities (See Table 3).
Table 2. Adjusted odds of depression and suicidality among lesbian, gay, and bisexual young adults ages 18–25 compared to straight peers
| Seriously considered suicide in past 12 months | Suicide plan in past 12 months | Suicide attempt in past 12 months | Major depressive episode in past 12 months | |||||
| aOR | 95% CI | aOR | 95% CI | aOR | 95% CI | aOR | 95% CI | |
| Gender (male ref) | ||||||||
| Female | 1.19 | 1.02–1.40 | 1.12 | .84–1.48 | 1.11 | 0.77–1.61 | 1.67 | 1.43–1.94 |
| Income (more than 2x poverty level ref) | ||||||||
| Up to 2x poverty threshold | 1.02 | 0.84–1.23 | 0.91 | .71–1.15 | 1.14 | 0.78–1.67 | 0.87 | .75–1.02 |
| Living in poverty | 1.01 | 0.86–1.2 | 1.10 | .87–1.39 | 0.97 | 0.67–1.41 | 0.92 | .77–1.09 |
| Race/Ethnicity (non-Hispanic White ref) | ||||||||
| Black/African American | 0.75 | 0.60–0.94 | 1.04 | .70–1.54 | 1.53 | .93–2.52 | 0.54 | 0.43–0.68 |
| American Indian/ Alaskan Native | 1.54 | 0.87–2.71 | 2.54 | 1.20–5.39 | 4.62 | 2.19–9.74 | 0.94 | 0.50–1.79 |
| Pacific Islander | 0.26 | 0.05–1.29 | NA | NA | NA | NA | 0.39 | 0.11–1.36 |
| Asian | 0.67 | 0.45–0.97 | 0.66 | .36–1.20 | 0.59 | 0.24–1.41 | 0.64 | 0.50–0.83 |
| More than one race | 1.46 | 1.03–2.05 | 2.18 | 1.33–3.55 | 2.61 | 1.43–4.79 | 1.18 | 0.83–1.70 |
| Hispanic | 0.71 | 0.58–0.86 | 0.91 | .68–1.23 | 1.23 | 0.79–1.92 | 0.81 | 0.67–0.97 |
| Sexual Identity(straight ref) | ||||||||
| LGB | 3.60 | 3.01–4.31 | 4.09 | 3.06–5.46 | 4.27 | 2.86–6.36 | 3.20 | 2.68–3.81 |
Table 3. Adjusted odds of depressive symptoms and suicidality among lesbian, gay, and bisexual high school students compared to straight peers
| Seriously considered suicide in past 12 months | Made a suicide plan in past 12 months | Attempted suicide in past 12 months | Depressive symptoms in past 12 months | |||||
| AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | |
| Gender (male ref) | ||||||||
| Female | 1.81 | 1.59–2.05 | 1.65 | 1.42–1.92 | 1.66 | 1.25–2.20 | 2.44 | 2.22–2.68 |
| Race/Ethnicity (non-Hispanic White ref) | ||||||||
| Black/African American | 0.63 | 0.54–0.75 | 0.79 | 0.57–1.10 | 1.28 | 0.86–1.89 | 0.81 | 0.66–0.99 |
| American Indian/Alaskan Native | 1.32 | 0.64–2.76 | 1.08 | 0.51–2.27 | 0.92 | 0.22–3.87 | 1.39 | 0.67–2.88 |
| Pacific Islander | 1.21 | 0.90–1.62 | 2.04 | 1.14–3.66 | 1.77 | 0.78–4.04 | 0.96 | 0.59–1.55 |
| Asian | 0.97 | 0.70–1.35 | 1.38 | 0.92–2.09 | 0.93 | 0.36–2.39 | 1.07 | 0.86–1.32 |
| More than one race | 1.28 | 0.95–1.72 | 1.62 | 1.22–2.14 | 1.68 | 1.21–2.33 | 1.36 | 1.05–1.75 |
| Hispanic | 0.87 | 0.78–0.97 | 1.02 | 0.83–1.23 | 1.30 | 0.92–1.82 | 1.15 | 1.01–1.31 |
| Sexual Identity(straight as ref) | ||||||||
| LGB | 5.26 | 4.44–6.22 | 4.78 | 3.86–5.91 | 4.42 | 3.25–6.01 | 3.76 | 3.20–4.42 |
LOOKING AHEAD
These data highlight the need for suicide prevention strategies focused on LGB youth from adolescence into young adulthood. With more than 1.8 million LGBTQ youth ages 13–24 seriously considering suicide each year (Green, Price-Feeney, & Dorison, 2019), it is imperative to address suicidality across the full age range. Below we outline implications for research, advocacy, and practice based on our findings. We also highlight implications specific to The Trevor Project.
Implications for Research. There is limited nationwide data examining suicidality across the lifespan, particularly specific to LGBTQ individuals. Similarly, existing studies have shortcomings with respect to how sexual identity was assessed and the inclusion of gender identity. Enhanced national data collection on sexual identity and gender identity, as well as suicidality, would allow greater understanding of disparities across different LGBTQ youth identities, including attention to how the intersectionality of multiple marginalized identities impacts suicidality. Additionally, there is an urgent need to develop and test novel prevention and intervention strategies for LGBTQ youth that are able to be successfully disseminated and implemented on a wide-scale.
Implications for Advocacy. These data highlight the need for LGBTQ-specific suicide prevention policies, funding streams dedicated to suicide prevention among LGBTQ youth, and advocacy efforts to improve sexual identity and gender identity data collection. Data on gender identity is lacking compared to data on sexual identity, and there is an urgent need to include measures of gender identity given the even greater disparities in suicidality among transgender and/or non-binary youth compared to cisgender youth (Price-Feeney, Green, & Dorison, In press). Additionally, the current data were based on suicidality outcomes among LGB youth, but not deaths by suicide, because reliable data are not available. It is critical that advocacy efforts focus on promoting the valid and reliable measurement of sexual identity and gender identity as part of violent death investigations in order to accurately understand factors related to the loss of young LGBTQ lives to suicide.
Implications for Practice. Despite recent strides in advancing LGBTQ rights, there are still astounding disparities in mental health among LGBTQ youth. These disparities highlight the need for LGBTQ-affirmative mental health services, particularly in regions of the U.S. where youth may have few treatment options. There is a need to enhance the LGBTQ-competence of community providers, including those who serve LGBTQ youth in school settings.
Implications for Trevor. These results motivate our commitment to save young LGBTQ lives. Importantly, these data fully support The Trevor Project’s focus on serving both LGBTQ youth and young adults in crisis. Because these findings document that disparities in suicidality persist for LGB youth beyond the age of 18, it is imperative that LGBTQ focused crisis services be available for young adults in addition to adolescents. And given the dearth of data on LGBTQ youth and young adults, these results also motivate Trevor’s continued research on suicidality among LGBTQ youth, so that we may better understand risk and protective factors and measure the impact of our efforts to end LGBTQ youth suicide.
This report is a collaborative effort from the following individuals at The Trevor Project:
| Amy Green, PhD Director of ResearchSamuel Dorison, LLM, MSc Chief Strategy & Innovation Officer | Myeshia Price-Feeney, PhD Research Scientist |
Recommended Citation: Green, A.E., Price-Feeney, M. & Dorison, S.H. (2019). Suicidality Disparities by Sexual Identity Persist from Adolescence into Young Adulthood. New York, New York: The Trevor Project.
| Media inquiries, please contact: Kevin Wong Head of Communications [email protected] 212.695.8650 x407 | For research-related inquiries, please contact: Amy Green, PhD Director of Research [email protected] 310.271.8845 x242 |
Download the PDF
References
Conner, K. R., Bridge, J. A., Davidson, D. J., Pilcher, C., & Brent, D. A. (2019). Meta-analysis of mood and substance use disorders in proximal risk for suicide deaths. Suicide and Life‐Threatening Behavior, 49(1), 278-292.
Curtin, S. C., & Heron, M. P. (2019). Death rates due to suicide and homicide among persons aged 10–24: United States, 2000–2017. National Center for Health Statistics Data Brief, 330, Hyattsville, MD: National Center for Health Statistics.
Dervic, K., Brent, D. A., & Oquendo, M. A. (2008). Completed suicide in childhood. Psychiatric Clinics of North America, 31(2), 271-291.
Grant, B. F., Saha, T. D., Ruan, W. J., Goldstein, R. B., Chou, S. P., Jung, J., … & Hasin, D. S. (2016). Epidemiology of DSM-5 drug use disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions–III. JAMA Psychiatry, 73(1), 39-47.
Green, A.E., Price-Feeney, M. & Dorison, S.H. (2019). National Estimate of LGBTQ Youth Seriously Considering Suicide. New York, New York: The Trevor Project.
Hedegaard H., Curtin S.C., & Warner M. (2018). Suicide mortality in the United States, 1999–2017. National Center for Health Statistics Data Brief, 330, Hyattsville, MD: National Center for Health Statistics.
Johns, M.M., Lowry, R., Andrzejewski, J., Barrios, L.C., Zewditu, D., McManus, T., et al. (2019). Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school student–19 states and large urban school districts, 2017. Morbidity and Mortality Weekly Report, 68(3), 65-71.
Johns M.M., Lowry R., Rasberry C.N., et al. (2018). Violence Victimization, Substance Use, and Suicide Risk Among Sexual Minority High School Students — United States, 2015–2017. Morbidity and Mortality Weekly Report, 67, 1211–1215
Kann L., Olsen E.O., McManus T., et al. (2016). Sexual Identity, Sex of Sexual Contacts, and Health-Related Behaviors Among Students in Grades 9–12 — United States and Selected Sites. 2015. Morbidity and Mortality Weekly Report Surveillance Summaries, 65, 1-202.
Meyer, I.H. (2003). Prejudice, social stress, and mental health in lesbian, gay, bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674-697.
Price-Feeney, M. Green, A.E., & Dorison, S.H. (In press). Understanding the mental health of transgender and nonbinary youth. Journal of Adolescent Health.
Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality (2019). 2018 National Survey on Drug Use and Health Data. Rockville, MD.
Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. (2014). The TEDS Report: Age of Substance Use Initiation among Treatment Admissions Aged 18 to 30. Rockville, MD.
The Trevor Project. (2019a). The Trevor Project research brief: Fostering the mental health of LGBTQ youth. Available at: https://www.thetrevorproject.org/2019/05/30/research-brief-fostering-the-mental-health-of-lgbtq-youth Accessed January 21, 2020.
The Trevor Project (2019b). National Survey on LGBTQ Mental Health. New York, New York: The Trevor Project.
© The Trevor Project 2021