Youth's Lives Every Day
EXECUTIVE SUMMARY
Environmental and community factors, defined in this report as the characteristics of the environment and community where a person lives, play an important role in the mental health of young people. However, there is very little research that examines the impact of community-level factors on the lives and mental health of LGBTQ young people. The American Community Survey (ACS), conducted by the United States (U.S.) Census Bureau, provides important community-level indicators, which can serve as environmental risk or protective factors for LGBTQ young people’s mental health. This report seeks to fill the gap in knowledge by examining community-level environmental indicators and their relationship with the mental health of LGBTQ young people using data from the ACS in conjunction with mental health indicators from The Trevor Project’s 2023 U.S. National Survey on the Mental Health of LGBTQ Young People.
Key Findings
Community-level environmental factors are significantly associated with the mental health of LGBTQ young people.
- LGBTQ young people living in communities where the median per capita income was above the national average reported lower rates of attempting suicide, compared to LGBTQ young people living in communities where the median per capita income was at or below the national average.
- LGBTQ young people living in communities where the community health insurance coverage was above the national average reported lower rates of attempting suicide compared to LGBTQ young people living in communities where the community health insurance coverage was at or below the national average.
- LGBTQ young people living in communities where the proportion of people who were born outside the U.S. was above the national average (i.e. communities with more immigrants) reported lower rates of attempting suicide, compared to LGBTQ young people living in communities where the proportion of people who were born outside the U.S. was at or below the national average.
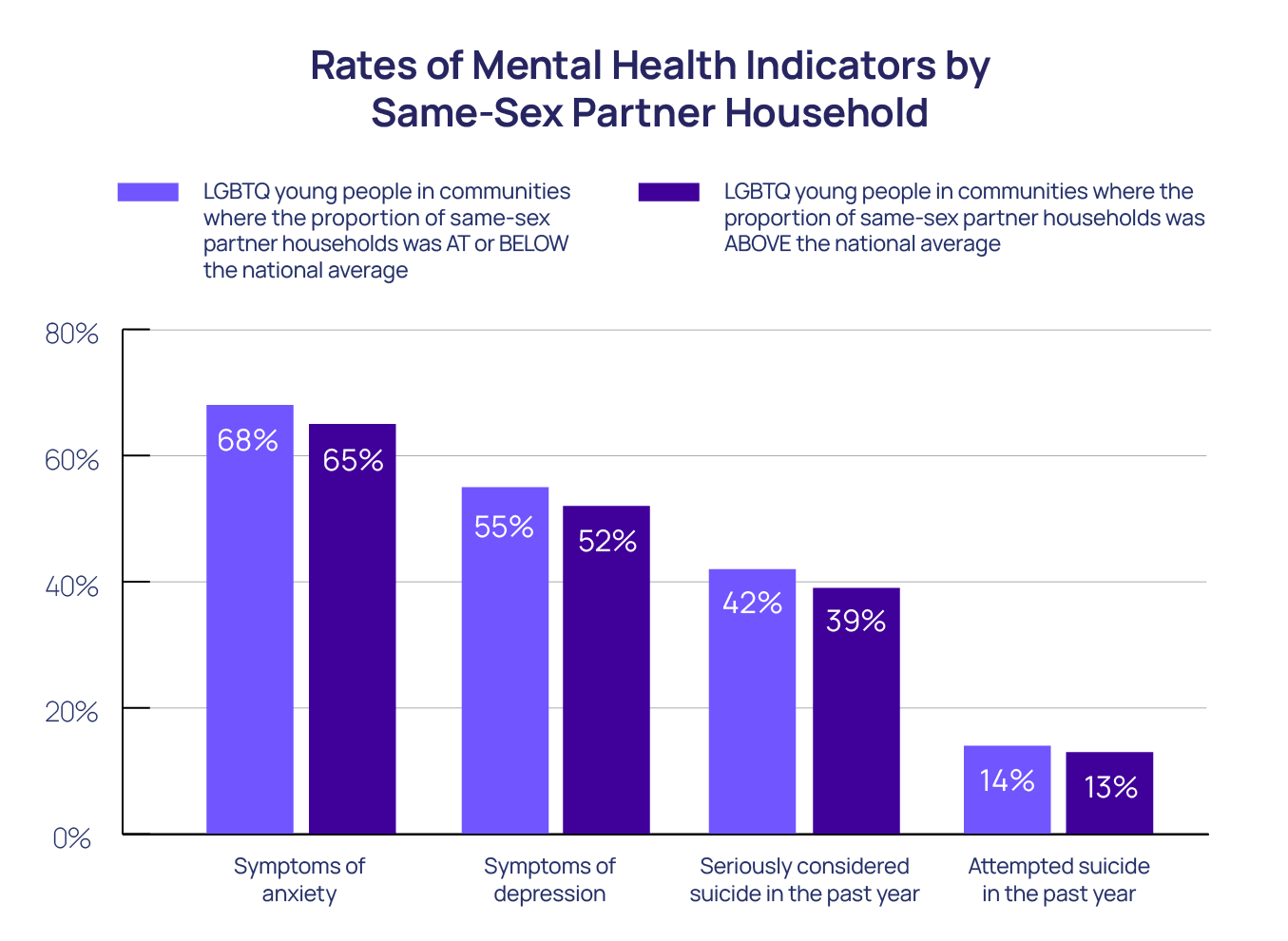
- LGBTQ young people living in communities where the proportion of same-sex partner households was above the national average reported lower rates of attempting suicide in the past year compared to LGBTQ young people living in communities where the proportion of same-sex partner households was at or below the national average.
- LGBTQ young people living in communities where the proportion of people of color was above the national average reported lower rates of attempting suicide compared to LGBTQ young people living in communities where the proportion of people of color was at or below the national average.
There are racial differences in the community-level factors where LGBTQ young people live.
- LGBTQ young people who reported being Native/Indigenous, White, and more than one race/ethnicity reported the highest rates of living in communities where the total community population was at or below the national average.
- Native/Indigenous, Hispanic/Latinx, and Black LGBTQ young people reported the highest rates of living in communities where both the per capita income and health insurance coverage were at or below the national average.
- Black LGBTQ young people reported the lowest rates of living in communities where the proportion of people of color was at or below the national average.
- Native/Indigenous and White LGBTQ young people reported the highest rates of living in communities where the proportion of people born outside the U.S. was at or below the national average.
- Native/Indigenous and Hispanic/Latinx LGBTQ young people reported the highest rates of living in communities where private school enrollment was at or below the national average.
Methodology Summary
A quantitative cross-sectional design was used to collect data for the 2023 U.S. National Survey on the Mental Health of LGBTQ Young People, using an online survey platform between September and December 2022. The final analytical sample included 28,524 LGBTQ young people between the ages of 13 and 24 from across the U.S. The questionnaire included up to 158 questions including zip code, race/ethnicity, and those assessing mental health. The mental health survey items included recent symptoms of anxiety and depression assessed with the GAD-2 and PHQ-2, respectively, as well as seriously considering and attempting suicide in the past year using questions taken from the Centers for Disease Control and Prevention’s (CDC) Youth Risk Behavior Survey. The ACS is a nationwide annual survey conducted by the U.S. Census that collects and produces information about communities in the U.S. The zip code-level environmental indicators in the ACS were joined with The Trevor Project’s U.S. National Survey on the Mental Health of LGBTQ Young People using the 5-digit zip codes self-reported by LGBTQ young people. The ACS indicators include zip code-level metrics for total population, median per capita income, and the proportions of: people 6 to 25 years old having health insurance coverage; people who identified as only White; people who are born outside the U.S.; same-sex partners in households; private and public school enrollments; and, labor force in military service. Chi-square and logistic regression analyses were used to examine differences among groups. Adjusted odds ratios predicting mental health indicators controlled for sex assigned at birth, gender identity, sexual orientation, race/ethnicity, and age. All reported comparisons are statistically significant at least at p<0.05. This means that there is less than a 5% probability each of these results occurred by chance.
Recommendations
This report found that community-level indicators are related to the mental health of LGBTQ young people. LGBTQ young people living in areas with less access to insurance, fewer reported same-sex couples in households, fewer people who were born outside the U.S., and/or lower average income reported higher rates of poor mental health. Additionally, LGBTQ young people with multiple marginalized identities, such as LGBTQ young people of color, had higher rates of living in communities with these community-level indicators (e.g., less access to insurance, lower average income) that are related to poor mental health. Finally, LGBTQ young people living in areas with a predominantly White population had poorer mental health in comparison to their LGBTQ peers living in communities with more racial/ethnic diversity. Although all young people may face similar stressors related to being a young person, LGBTQ young people also experience risks that are specific to being LGBTQ, such as anti-LGBTQ victimization, which can place them at even higher risk for challenges to their mental health and well-being. Resources, such as healthcare and financial assistance programs, should be allocated to communities in greater need in order to prioritize LGBTQ young people and their mental health. Additionally, efforts to increase access to LGBTQ-affirming spaces and people in communities should be prioritized in order to provide effective support for LGBTQ young people.
BACKGROUND
Lesbian, gay, bisexual, transgender, queer, and questioning (LGBTQ) young people report higher rates of poor mental health and suicide risk than their straight, cisgender peers. LGBTQ young people report higher rates of anxiety, depression, seriously considering suicide, and attempting suicide when compared to straight and cisgender young people (Johns et al., 2020; Russell & Fish, 2016). Transgender and nonbinary young people report poorer mental health and higher suicide risk when compared to both cisgender young people (Johns et al., 2019) and cisgender LGBQ young people (Price-Feeney et al., 2020). These increased mental health risks are not due to young people’s LGBTQ identities, but rather the result of the increased stress, discrimination, and violence which they experience as they navigate anti-LGBTQ bias in society (Meyer, 2003; Velez et al., 2021). For example, LGBTQ young people may experience rejection from their families due to anti-LGBTQ beliefs, as well as anti-LGBTQ victimization, bullying, and/or discrimination (Kosciw et al., 2018; Ryan et al., 2009). These negative experiences can cause LGBTQ young people to internalize anti-LGBTQ sentiments and lead to feelings of perceived burdensomeness, which are associated with higher rates of suicidal ideation among LGBQ individuals (Baams et al., 2015; Hill & Petit, 2012).
Environmental and community factors play an important role in the mental health of young people in the United States. In this report, they are defined as the characteristics of the environment and community where a person lives. The characteristics of the environment where a young person grows up have long been shown to have effects on their development and mental health (Bronfenbrenner, 1994; Tudge et al., 2022). For example, living in a neighborhood with lower levels of social cohesion (i.e. the level of connectedness between individuals living in close geographical proximity) has been found to be associated with higher rates of poor mental health after a stressful life event among adolescents (Kingsbury et al., 2020). For LGBTQ young people, they often contend with both environmental factors, such as low social cohesion in their community, alongside their non-LGBTQ peers, in addition to LGBTQ-specific stressors. Therefore, any community-level factor that ameliorates LGBTQ-specific stressors is likely to be a strong protective factor for their mental health. For example, lesbian, gay, bisexual, and queer (LGBQ) students who live in more socially supportive communities (as determined by a composite measure which include metrics such as proportions of same-sex couples in their communities, or proportions of Gay-Straight Alliances in schools) report fewer suicide attempts than their peers living in socially unsupportive environments (Hatzenbuehler, 2011). Conversely, LGBQ young people who live in neighborhoods with higher recent LGBTQ-based hate crime rates report higher rates of considering or attempting suicide, compared to both straight young people living in those same neighborhoods and young people living in neighborhoods with lower recent LGBTQ hate crime rates (Duncan & Hatzenbuehler, 2014). Additionally, LGBQ young people living in counties with fewer LGBTQ-specific anti-bullying policies report higher odds of attempting suicide compared to those who lived in counties with more LGBTQ-specific anti-bullying policies (Hatzenbuehler & Keyes, 2013). The mental health of transgender and nonbinary young people is particularly impacted by community-level policies restricting their access to social transition, gender-affirming health care, and sex-segregated facilities, such as locker rooms or bathrooms (Flaskerud & Lesser, 2018). Transgender and nonbinary youth who live in states with fewer laws restricting the rights of LGBTQ people report higher rates of correct name and pronoun usage (Renley et al., 2022), which is in turn associated with better mental health (The Trevor Project, 2023; Pollitt et al., 2021).
The American Community Survey (ACS) provides important community-level indicators, which can serve as environmental risk or protective factors for LGBTQ young people’s mental health. Because the ACS does not ask respondents to directly report their sexual orientation or gender identity, and asks them if they are in a same-sex relationship instead, most research using ACS data has examined differences between adults in same-sex and opposite-sex relationships (Badgett et al., 2021). Overall, the ACS has been used to explore levels of education, health insurance coverage, and household income among adults in same-sex couples compared to adults in opposite-sex couples (Badgett et al., 2021; Gates, 2013; Jepsen & Jepsen, 2022); however, there has yet to be a study that uses ACS data to explore LGBTQ young people’s mental health.
While the field of suicide prevention research has largely focused efforts on individual and social influences, to date, it has yet to substantively examine the impact of the community on suicidality among LGBTQ young people. This may be due to a number of factors. Representative community-level sampling is very expensive and labor-intensive. For example, the proposed budget for the 2023 ACS is $235.6 million (U.S. Census Bureau, 2022). Suicide research is also historically underfunded, even in comparison to research on other mental health conditions (Reidenberg & Berman 2017). On top of that, LGBTQ individuals have traditionally been understudied in larger health surveillance surveys in the U.S., further exacerbating gaps in understanding about the mental health of LGBTQ young people (Durso, 2018). This report seeks to fill the gap in knowledge by examining community-level environmental indicators and their impact on mental health among 21,999 LGBTQ young people ages 13 to 24 in the U.S.
METHODOLOGY
The Trevor Project’s 2023 U.S. Survey on the Mental Health of LGBTQ Young People
Data were collected from an online survey platform between September and December 2022. LGBTQ young people between the ages of 13 and 24 were recruited via targeted ads on social media. The final analytical sample included 28,524 LGBTQ young people from across the U.S. The overall survey included a maximum of 158 questions. Mental health outcomes were measured using a variety of survey items. Current symptoms of anxiety were measured using the GAD-2 (Plummer et al., 2016), and current symptoms of depression were measured using the PHQ-2 (Richardson et al., 2010), which were both brief screeners. The established cutoff of a score greater than two on each measure was used to resemble having symptoms of anxiety or depression. Questions on considering suicide and attempting suicide in the past 12 months were taken from the CDC’s YRBS (Centers for Disease Control and Prevention, 2021). Race/ethnicity was collected from each survey participant by asking “What best describes your race or ethnicity?” with options: Asian/Asian American, Black/African American, Hispanic or Latino/Latinx, more than one race or ethnicity, Indigenous/Native, Pacific Islander/Native Hawaiian, White/Caucasian, and another race or ethnicity (please specify). Zip code data, a number that identifies individual postal service areas by the U.S. Postal Service, were also collected from each survey participant. Overall, 21,999 young people (77%) provided a valid 5-digit zip code, and are therefore included in the analyses.
Utilizing Statistics from the American Community Survey
The ACS is a nationwide annual survey that collects and produces information on social, economic, housing, and demographic characteristics about the communities in the U.S. Each year, the U.S. Census Bureau contacts over 3.5 million households across the U.S. to participate. Community-level environmental indicators at the zip code level were obtained from the 2017-2021 ACS (Manson et al., 2022).
Out of over 1,000 possible neighborhood indicators, eight community-level environmental indicators were chosen for inclusion in the current report due to their potential relationship to mental health and well-being among LGBTQ young people:
- Total population
- Median per capita income
- Health insurance coverage for people 6 to 25 years old
- Race/ethnicity
- The proportion of people who were born outside the U.S.
- The proportion of same-sex partner households
- School enrollment type (private vs. public)
- The proportion of the labor force in military service.
All measures on the ACS were dichotomized to provide categories that were above the national mean, or henceforth average, compared to at or below the national average for that specific indicator, as aggregated from the original ACS data for that indicator. Additionally, the racial/ethnic diversity of a community was measured by the proportion of racial/ethnic minority in a community (i.e. the proportion of people of color in a community was “above” or “at or below” the national average). To evaluate the mental health of LGBTQ young people of color who live in a community predominantly composed of White individuals, we grouped all LGBTQ young people who did not identify as exclusively White, which included Asian American/Pacific Islander (AAPI), Black, Hispanic/Latinx, Middle Eastern/Northern African (MENA), Native/Indigenous, and young people who identified with more than one race/ethnicity.
The two datasets were combined by matching ACS data and the 5-digit zip code reported by LGBTQ young people in the 2023 U.S. National Survey on the Mental Health of LGBTQ Young People. Chi-square and logistic regression analyses were used to examine differences in groups (by community-level indicator, race/ethnicity, sexual orientation, and gender identity) and to determine the adjusted odds of mental health indicators. Adjusted odds ratios predicting mental health indicators controlled for sex assigned at birth, gender identity, sexual orientation, race/ethnicity, and age. The comparisons for racial/ethnic, sexual orientation, and gender identity differences examined each identity individually without further grouping. Racial/ethnic differences included all response options from the previous paragraph; sexual orientation included asexual, bisexual, gay, lesbian, pansexual, queer, and questioning; gender identity included cisgender boy/man, cisgender girl/woman, nonbinary/genderqueer, questioning, transgender boy/man, and transgender girl/woman. All reported comparisons are statistically significant at least at p<0.05. This means that there is less than a 5% probability each of these results occurred by chance.
RESULTS
Sample Demographics
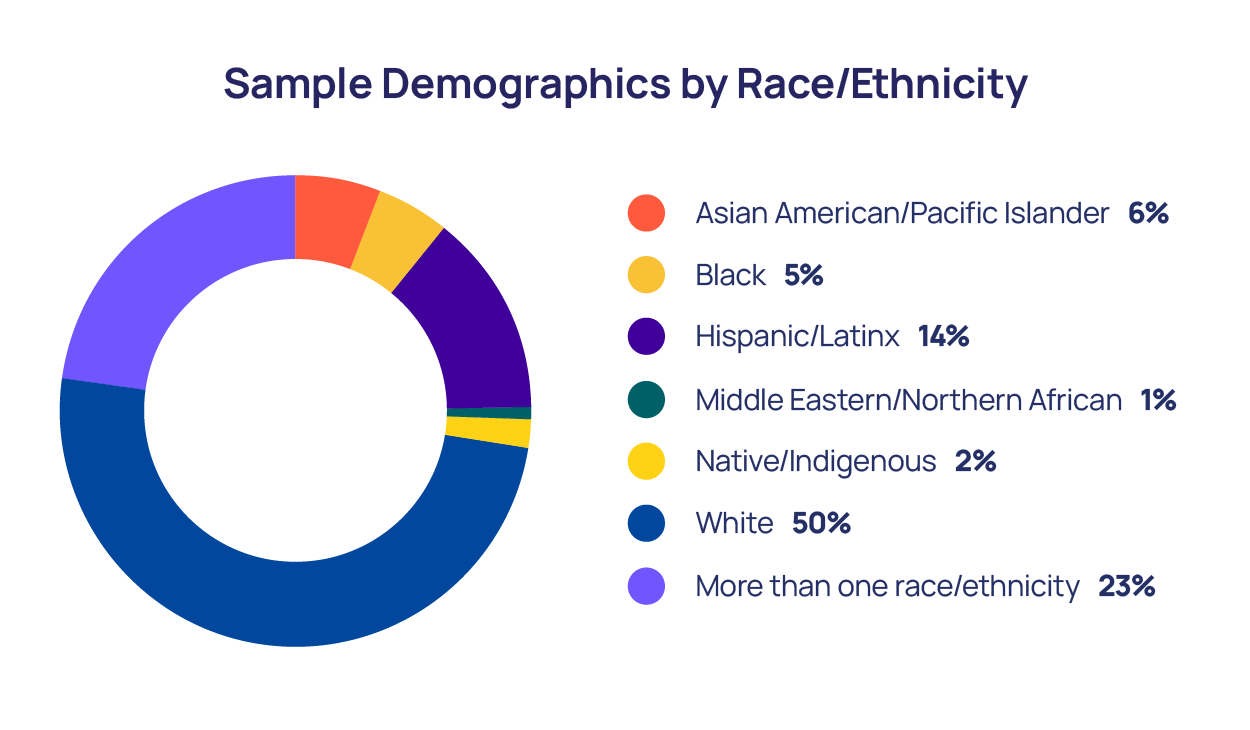
In our sample, 6% of LGBTQ young people identified as Asian American/Pacific Islander, 5% as Black, 14% as Hispanic/Latinx, 1% as Middle Eastern/Northern African, 2% as Native/Indigenous,, 50% as White, and 23% identified as more than one race/ethnicity.
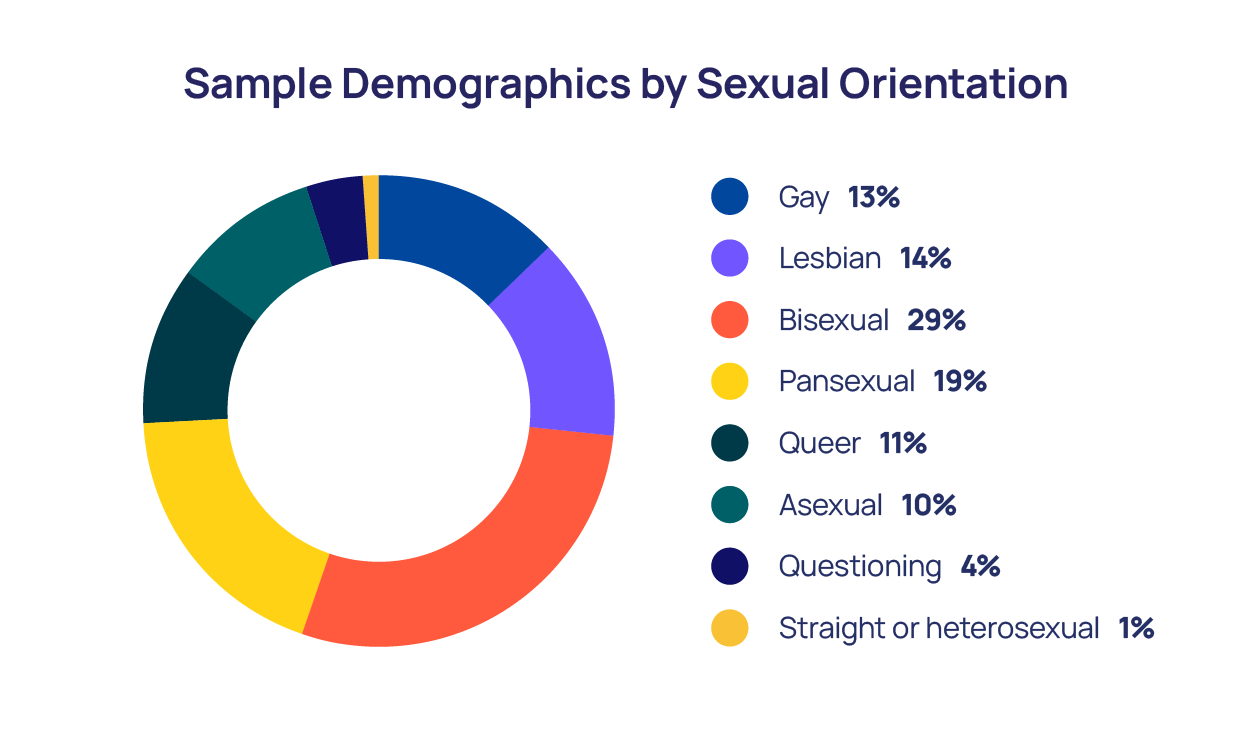
Sexual orientation data showed that 13% of LGBTQ young people in our sample identified as gay, 14% as lesbian, 29% as bisexual, 11% as queer, 19% as pansexual, 10% as asexual, 4% as questioning, and 1% identified as straight or heterosexual.
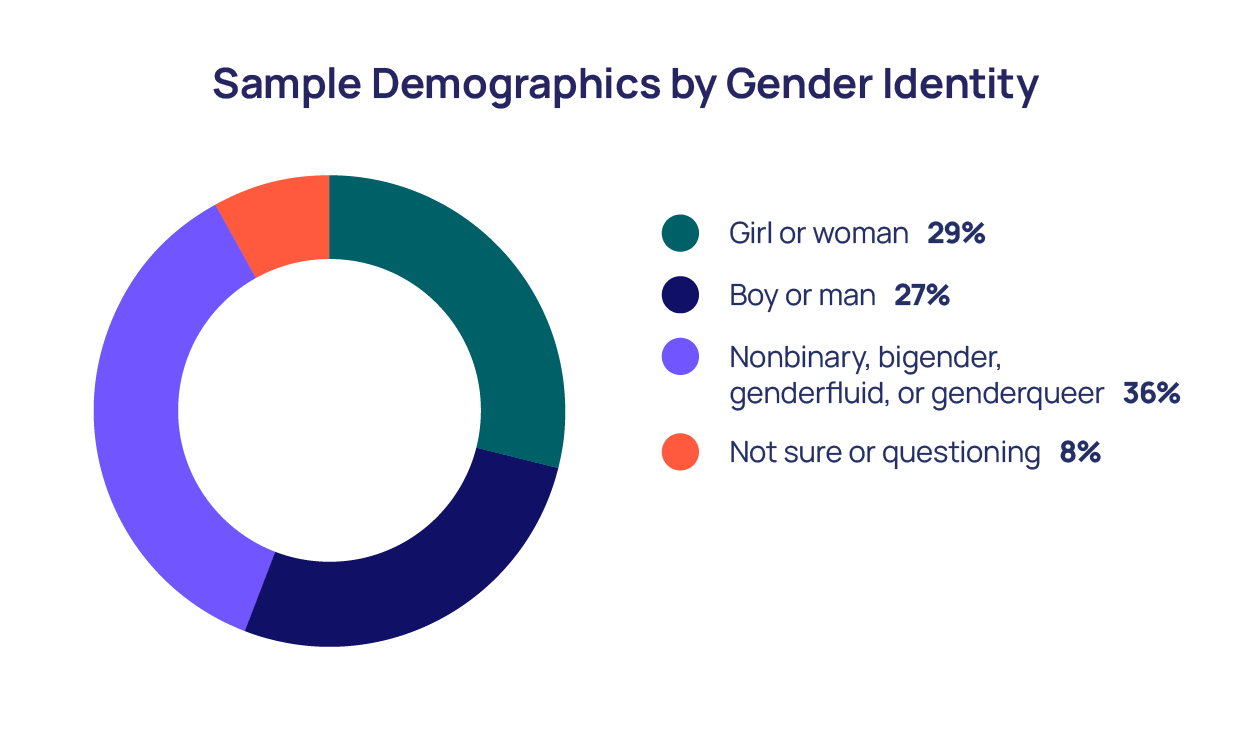
Twenty-nine percent of LGBTQ young people identified as a girl or woman, 27% identified as a boy or man, 36% identified as nonbinary, bigender, genderfluid or genderqueer, and 8% identified as not sure or questioning. Overall, 41% of LGBTQ young people in our sample identified as cisgender, and 51% as transgender or nonbinary.
The majority of LGBTQ young people in our sample reported currently living in a home with one or more parent or guardian (74%). Other living arrangements included: 6% in a home with roommates; 5% in college housing; 4% in a home with a significant other; 4% in another relative’s home; 3% in other living arrangements; 3% living alone; and, 1% in temporary or transitional housing (e.g., friend’s home, shelters, cars, campgrounds, foster homes, group homes, or hotels/motels).
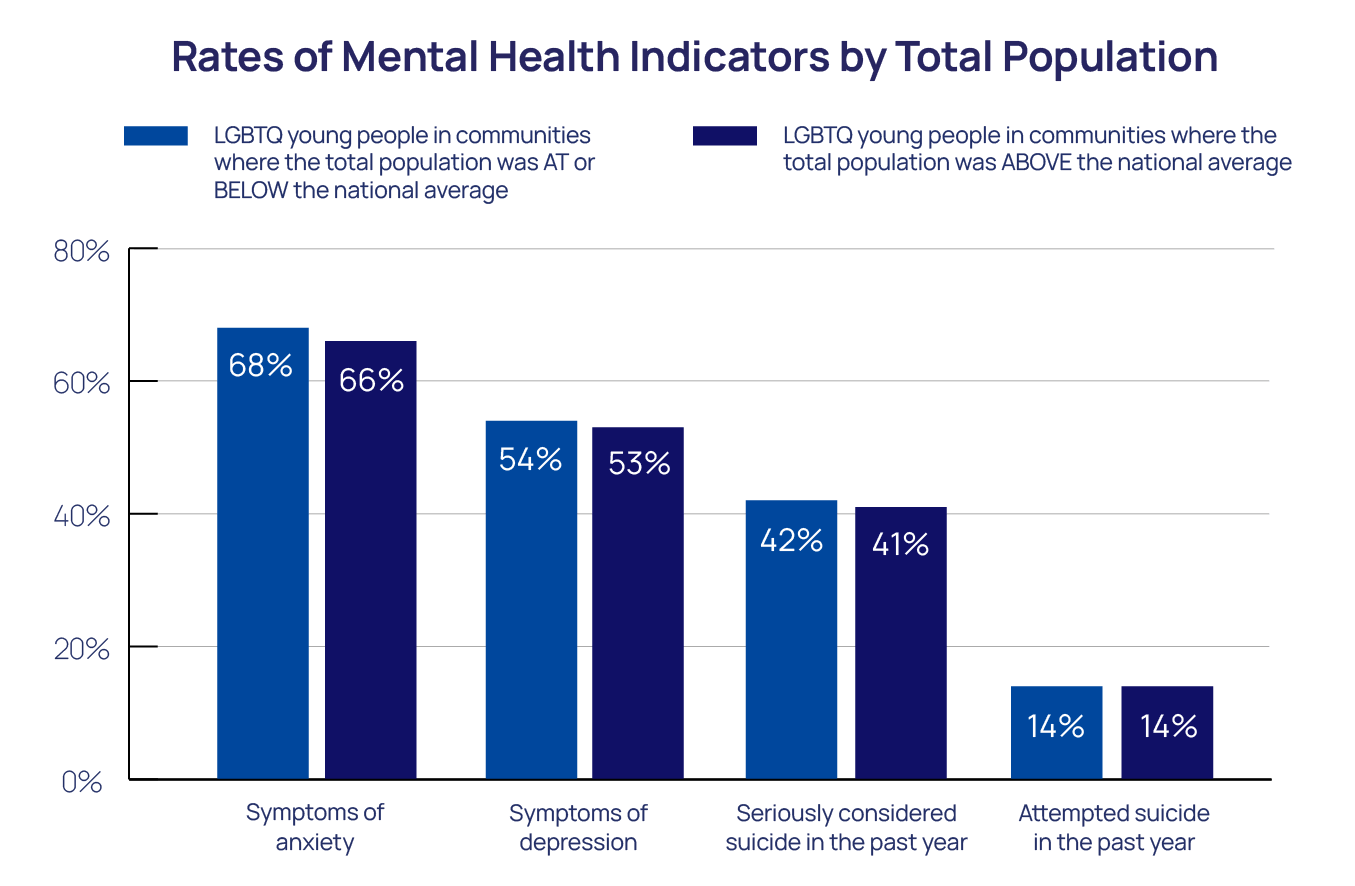
Total Community Population
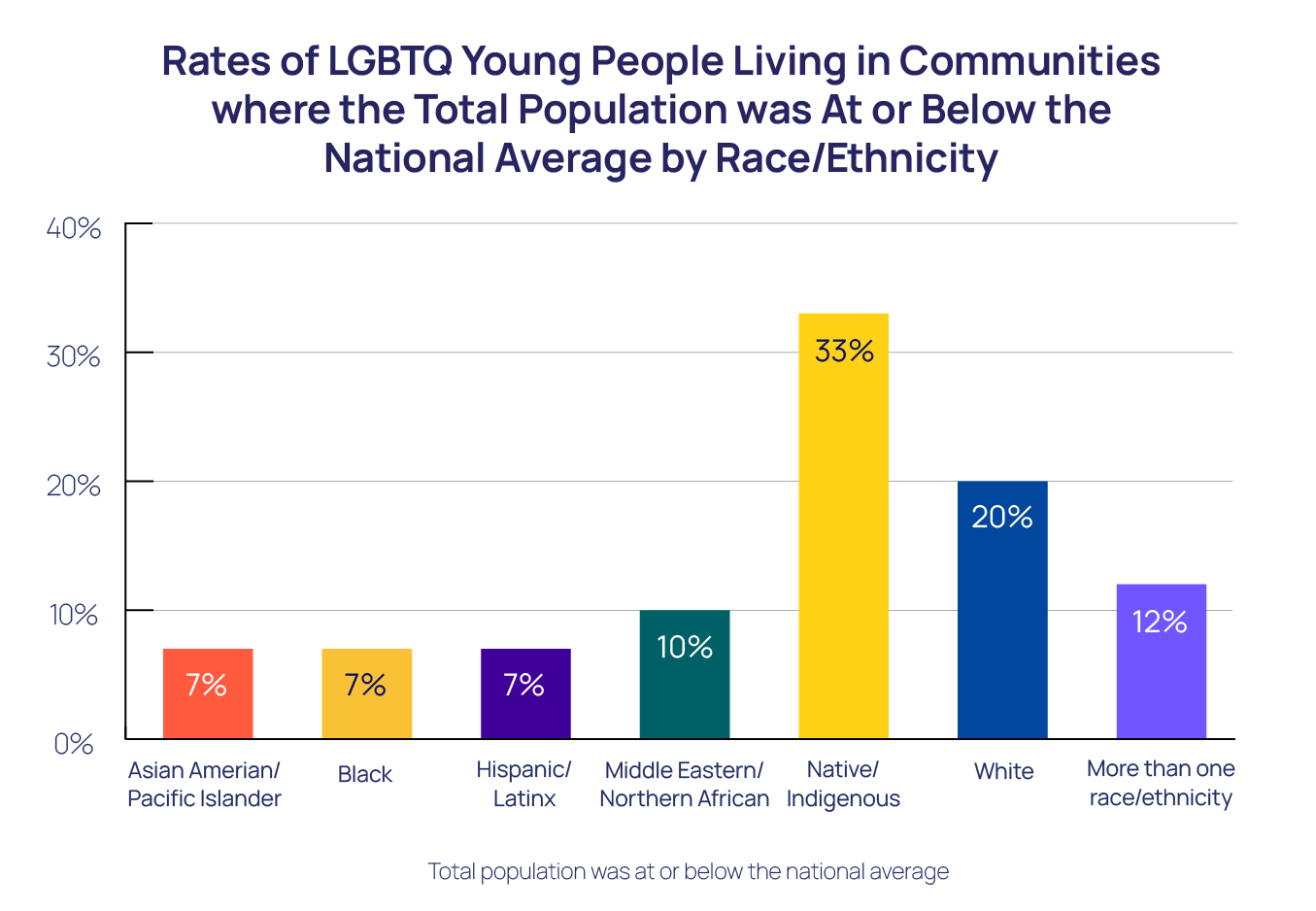
Total community population provides information about the number of people living in a community. LGBTQ young people may have more access to positive role models (Bird et al., 2012) and community-level resources in larger, often urban, communities (Ellis et al., 2009). Racial differences exist among LGBTQ young people in regard to the community they live in. LGBTQ young people who identified as Native/Indigenous, White, and more than one race/ethnicity reported living in communities where the total population was at or below the national average at significantly higher rates, compared to LGBTQ young people of other races/ethnicities. There were no differences among LGBTQ young people across sexual orientation or gender identity.
Overall, LGBTQ young people living in communities where the total population was above and at or below the national average reported similar rates of mental health indicators. However, one notable exception demonstrated that LGBTQ young people living in communities where the total population was above the national average had lower rates of symptoms of anxiety, compared to LGBTQ young people living in communities where the total population was at or below the national average(66% compared to 68%, p < 0.05).
Community Per Capita Income
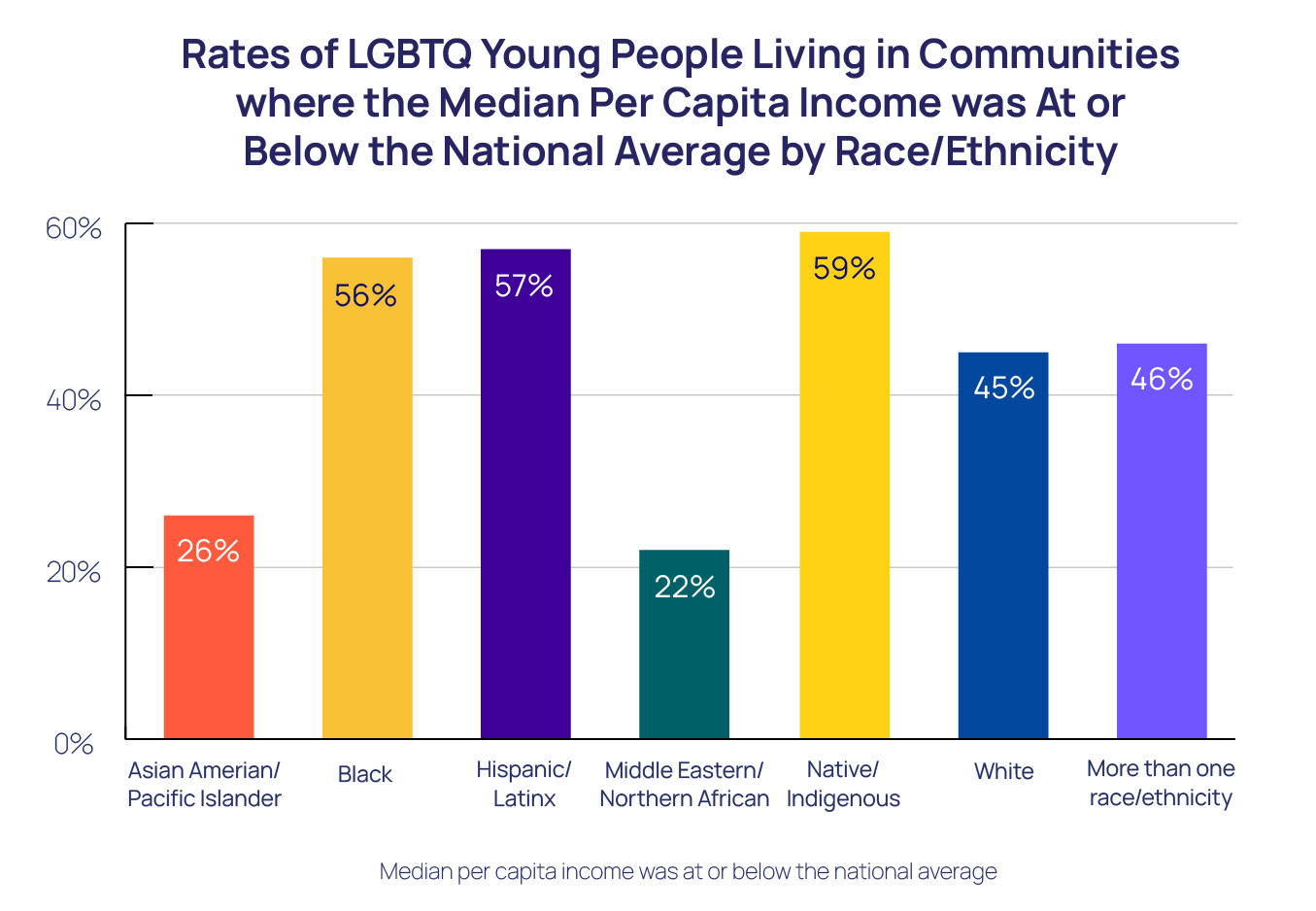
Per capita income is the average income earned per person in a given area, and it represents the average income level of people living in a community. In communities with higher per capita income, there may be greater financial resources to provide extra community-level support, such as LGBTQ resource centers or mental health professionals (Ellis et al., 2009). There were racial differences wherein Native/Indigenous, Hispanic/Latinx, and Black LGBTQ young people reported significantly higher rates of living in communities where the median per capita income was at or below the national average, compared to LGBTQ young people of other races/ethnicities . There were no differences among LGBTQ young people across sexual orientation or gender identity.
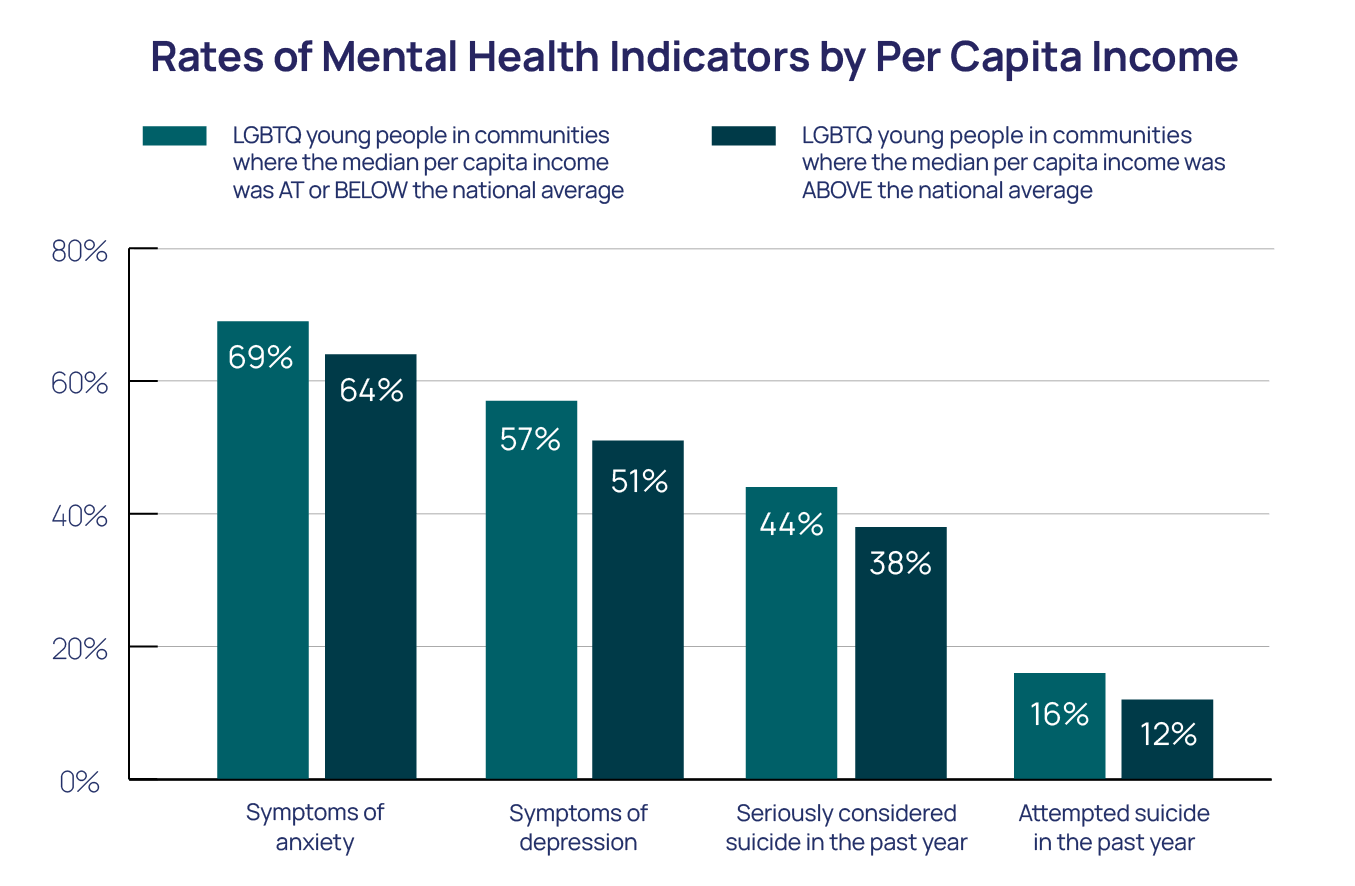
Overall, LGBTQ young people living in communities where the median per capita income was above the national average reported better mental health indicators, compared to LGBTQ young people living in communities at or below the national average of per capita income. LGBTQ young people living in communities where the per capita income was above the national average reported significantly lower rates of symptoms of anxiety (64% compared to 69%, p < 0.01), symptoms of depression (51% compared to 59%, p < 0.01), seriously considering suicide in the past year (38% compared to 44%, p < 0.01), and attempting suicide in the past year (12% compared to 16%, p < 0.01). Specifically, LGBTQ young people living in communities where the median per capita income was above the national average had 24% lower odds of reporting an attempted suicide in the past year (aOR=0.76, 95% CI [0.70, 0.82]), compared to LGBTQ young people living in communities where the median per capita income was at or below the national average.
Community Health Insurance Coverage
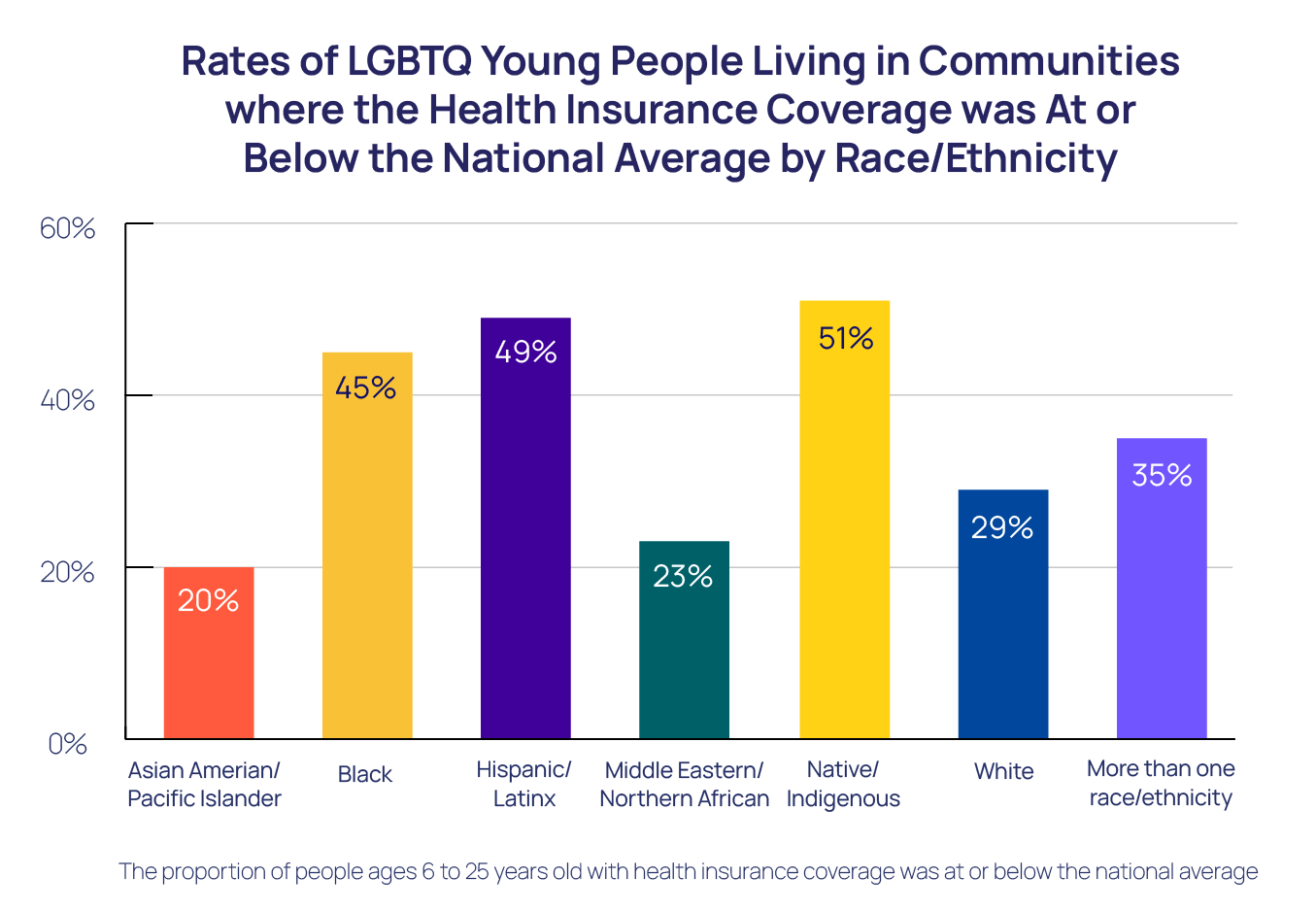
Health insurance coverage provides insights on the accessibility of healthcare within a community. Communities with higher health insurance coverage may have more access to proper physical and mental health care (American Hospital Association, 2022). Racial differences exist in communities where LGBTQ young people reside in terms of health care coverage. Native/Indigenous, Hispanic/Latinx, and Black LGBTQ young people reported significantly higher rates of living in communities where the proportion of people ages 6 to 25 years old with health insurance coverage was at or below the national average, compared to LGBTQ young people of other races/ethnicities. There were no differences among LGBTQ young people across sexual orientation or gender identity.
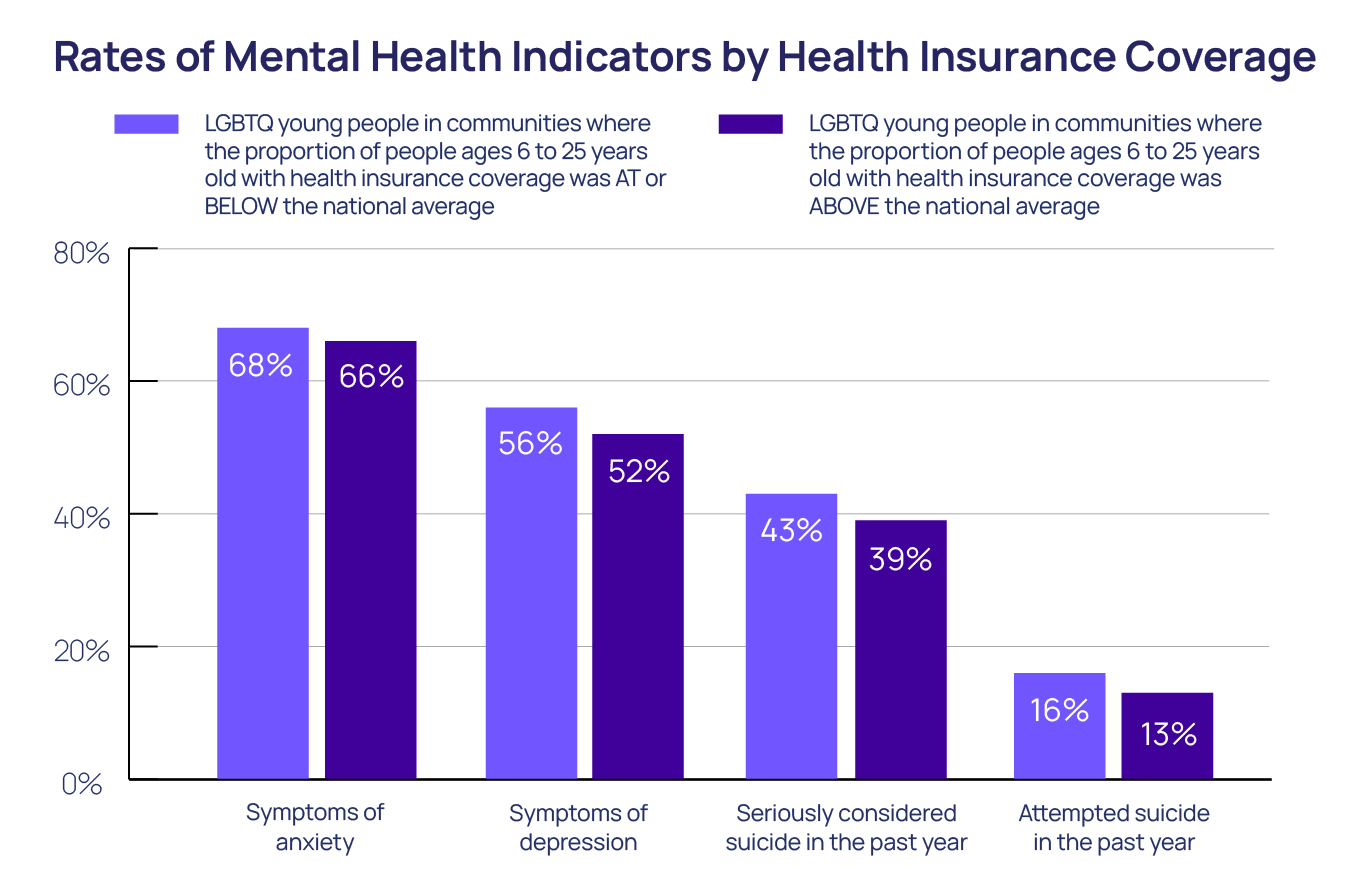
Overall, LGBTQ young people living in communities where the proportion of people ages 6 to 25 years old with health insurance coverage was above the national average reported better mental health, compared to LGBTQ young people living in communities where the proportion of people ages 6 to 25 years old with health insurance coverage was at or below the national average. LGBTQ young people living in communities where the proportion of people ages 6 to 25 years old with health insurance coverage was above the national average reported significantly lower rates of symptoms of anxiety (66% compared to 68%, p < 0.01), symptoms of depression (52% compared to 56%, p < 0.01), seriously considering suicide in the past year (39% compared to 43%, p < 0.01), and attempting suicide in the past year (13% compared to 16%, p < 0.01). Indeed, LGBTQ young people living in communities where the proportion of people ages 6 to 25 years old with health insurance was above the national average had 18% lower odds of reporting an attempted suicide in the past year (aOR=0.82, 95% CI [0.75, 0.89]), compared to LGBTQ young people living in communities where the proportion of people ages 6 to 25 years old with health insurance was at or below the national average.
Community Proportion of Racial/Ethnic Minority
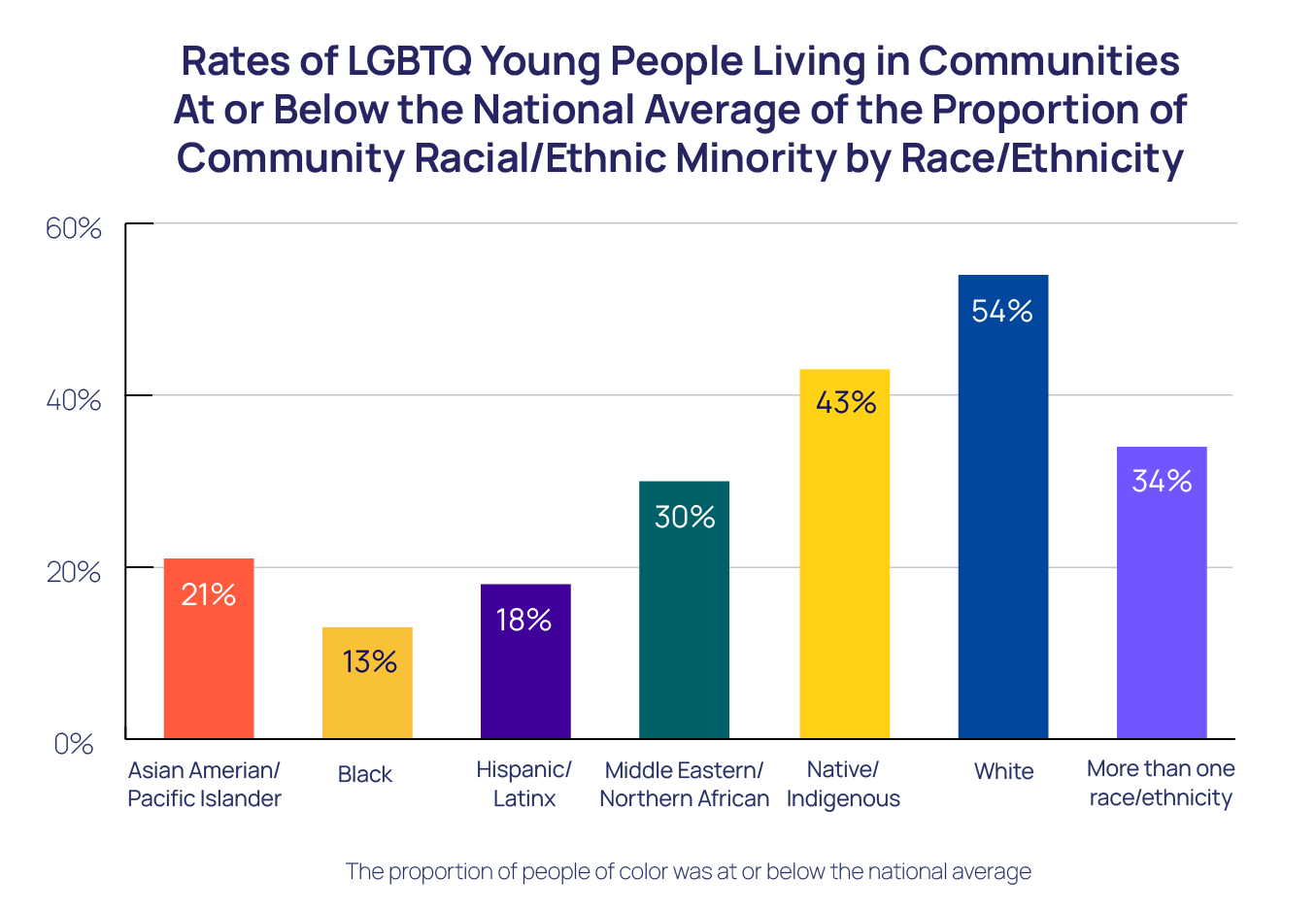
Community proportion of racial/ethnic minority measures how racially/ethnically diverse a community is. This report adopts a narrow definition of racial/ethnic diversity, and reports the proportion of people within a community who reported being a person of color. People living in racially/ethnically diverse communities may experience lower rates of racial discrimination (Dailey et al., 2010) or may be more likely to accept people outside of their own identities (Bai et al., 2020). There is a racial difference wherein Black LGBTQ young people reported significantly lower rates of living in communities where the proportion of people of color in the community was at or below the national average (i.e., less White communities), compared to LGBTQ young people of all other races/ethnicities. There were no differences among LGBTQ young people across sexual orientation or gender identity.
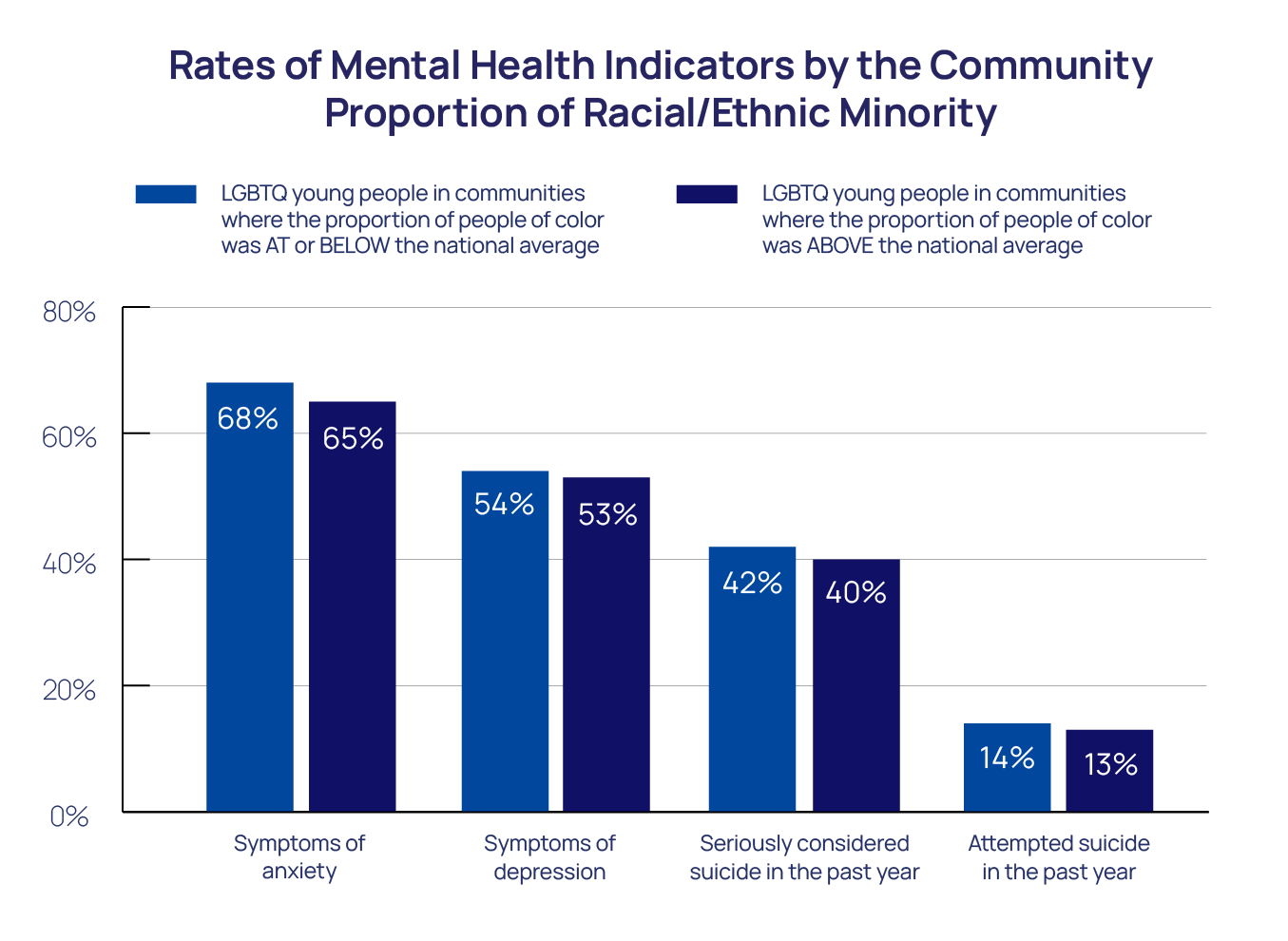
Overall, LGBTQ young people living in communities where the proportion of people of color was above the national average reported better mental health outcomes, compared to LGBTQ young people living in communities where the proportion of people of color was at or below the national average. LGBTQ young people living in communities where the proportion of people of color was above the national average reported lower rates of symptoms of anxiety (65% compared to 68%, p < 0.01), symptoms of depression (53% compared to 54%, p < 0.05), and seriously considering suicide in the past year (40% compared to 42%, p < 0.01). However, the rates of attempting suicide in the past year were similar to LGBTQ young people living in communities where the proportion of people of color was above the national average.
Importantly, the finding that LGBTQ young people living in communities where the proportion of people of color was above the national average reported lower rates of poor mental health indicators was true for both LGBTQ youth of color and White LGBTQ youth living in those communities.
Proportion of People Born Outside of the U.S.
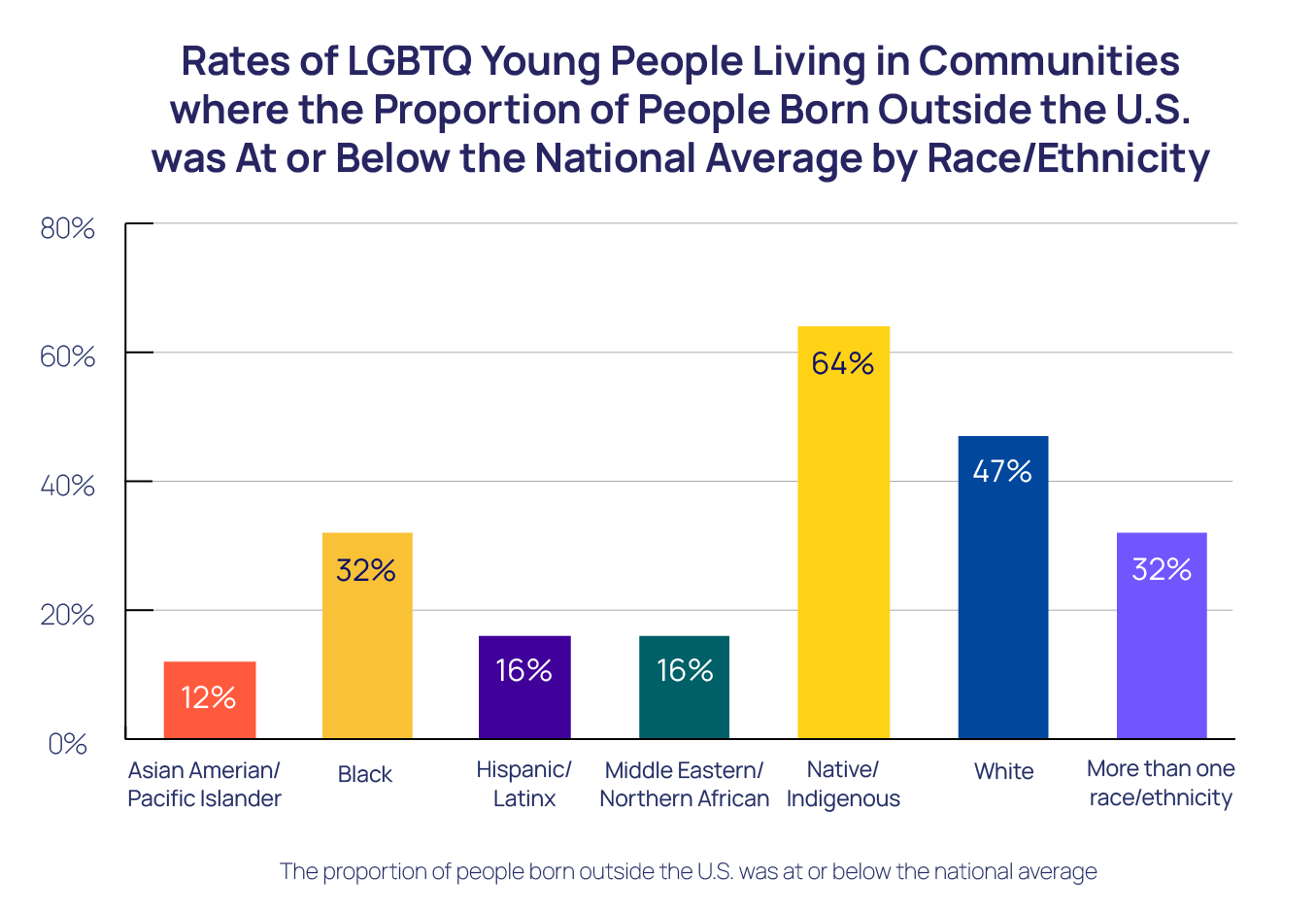
Nativity highlights the proportion of people who were born in the U.S. compared to people who were born outside the U.S. within a community. LGBTQ young people living in communities with higher proportions of people born outside the U.S. may have greater access to culturally driven protective social resources, such as a collective sense of community identity or extended familial support (Lau et al., 2013). There were racial differences in which Native/Indigenous and White LGBTQ young people reported significantly higher rates of living in communities where the proportion of people who were born outside the U.S. was at or below the national average, compared to LGBTQ young people of all other races/ethnicities. There were no differences among LGBTQ young people across sexual orientation or gender identity.
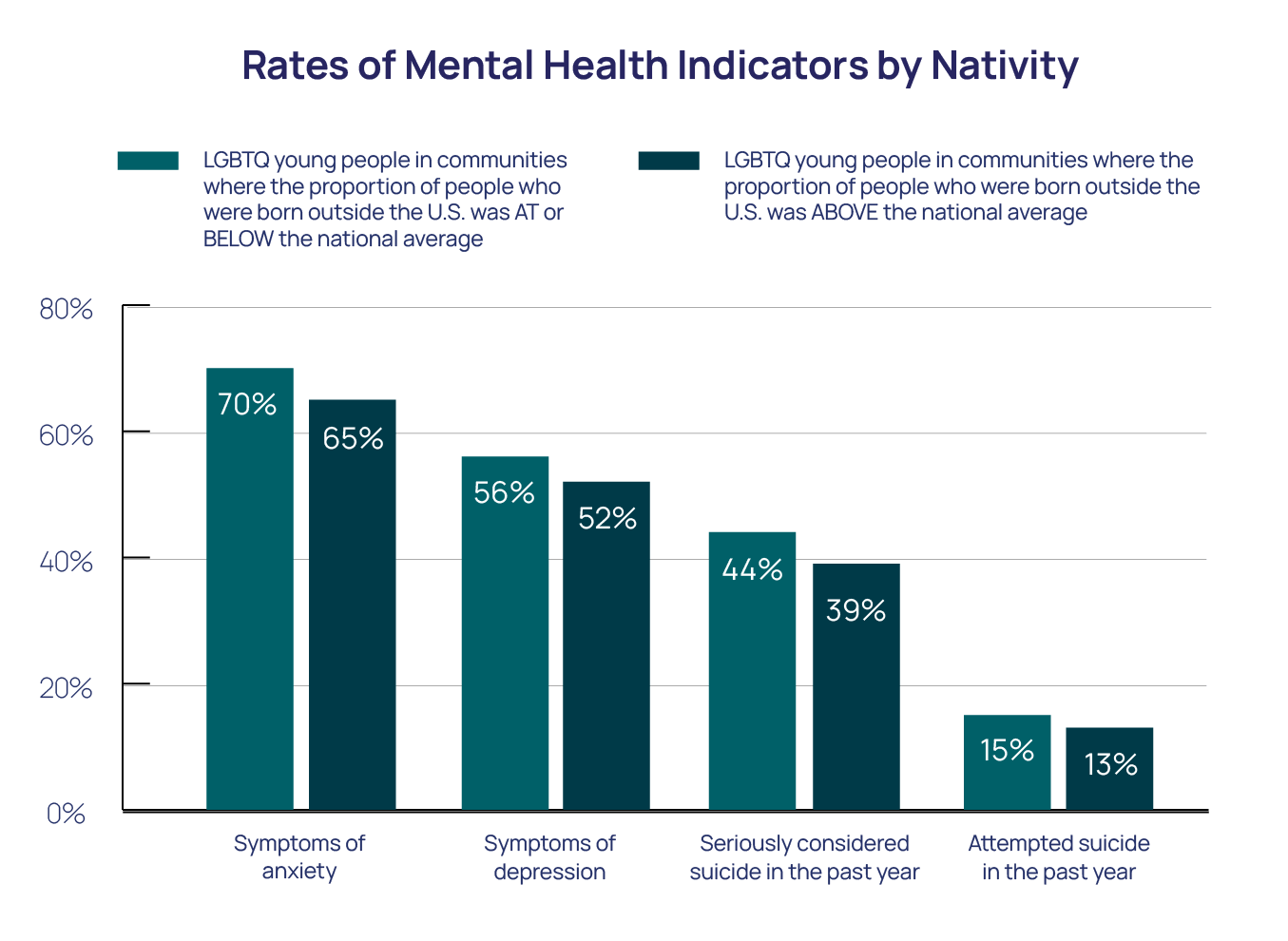
Overall, LGBTQ young people living in communities where the proportion of people who were born outside the U.S. was above the national average reported better mental health outcomes, compared to LGBTQ young people living in communities where the proportion of people who were born outside the U.S. was at or below the national average. LGBTQ young people living in communities where the proportion of people who were born outside the U.S. was above the national average reported significantly lower rates of symptoms of anxiety (65% compared to 70%, p < 0.01), symptoms of depression (52% compared to 56%, p < 0.01), seriously considering suicide in the past year (39% compared to 44%, p < 0.01), and attempting suicide in the past year (13% compared to 15%, p < 0.01). Notably, LGBTQ young people living in communities where the proportion of people who were born outside the U.S. was above the national average had 24% lower odds of reporting an attempted suicide in the past year (aOR=0.76, 95% CI [0.69, 0.83]), compared to LGBTQ young people living in communities where the proportion of people who were born outside the U.S. was at or below the national average.
Proportion of Same-Sex Partner Households
The proportion of same-sex partner households measures the level of same-sex couple representation within a community. It may be related to LGBTQ young people’s mental health, as LGBTQ young people living in communities with a higher proportion of same-sex partner households may have more access to role models and see themselves reflected in a positive way (Bird et al., 2012). There were no differences among LGBTQ young people across race, sexual orientation, or gender identity with regard to the proportion of same-sex partner households in communities in which they live.
Overall, LGBTQ young people living in communities where the proportion of same-sex partner households was above the national average reported better mental health outcomes compared to LGBTQ young people living in communities where the proportion of same-sex partner households was at or below the national average. LGBTQ young people living in communities where the proportion of same-sex partner households was above the national average reported significantly lower rates of symptoms of anxiety (65% compared to 68%, p < 0.01), symptoms of depression (52% compared to 55%, p < 0.01), seriously considering suicide in the past year (39% compared to 42%, p < 0.01), and attempting suicide in the past year (13% compared to 14%, p < 0.01). Specifically, LGBTQ young people living in communities where the proportion of same-sex partner households was above the national average had 9% lower odds of reporting a suicide attempt in the past year (aOR=0.91, 95% CI [0.84, 0.99]), compared to LGBTQ young people living in communities where the proportion of same-sex partner households was at or below the national average.
Community School Enrollment Type
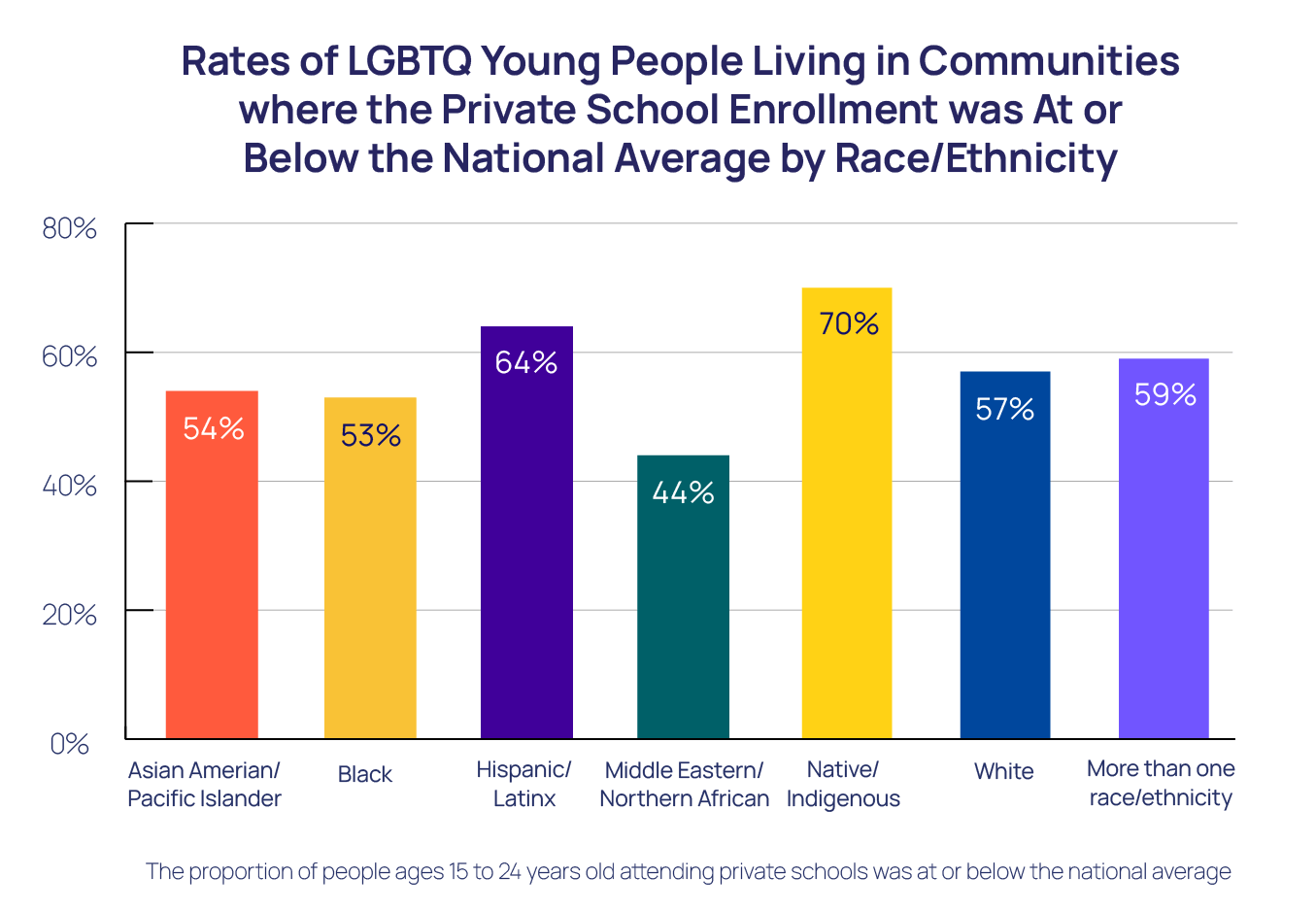
The indicator for school enrollment allows for comparison between communities based on the rates of private school enrollment and public school enrollment. Similar to people living in communities with high per capita income, people living in communities with high private school enrollment may have additional family wealth and financial ability to provide community-level resources (Yeung & Conley, 2008). All school levels are accounted for, including college enrollment. There were racial differences with Native/Indigenous and Hispanic/Latinx LGBTQ young people reporting significantly higher rates of living in communities where the proportion of people ages 15 to 24 years old attending private schools was at or below the national average, compared to LGTBQ young people of all other races/ethnicities. There were no differences among LGBTQ young people across sexual orientation or gender identity.
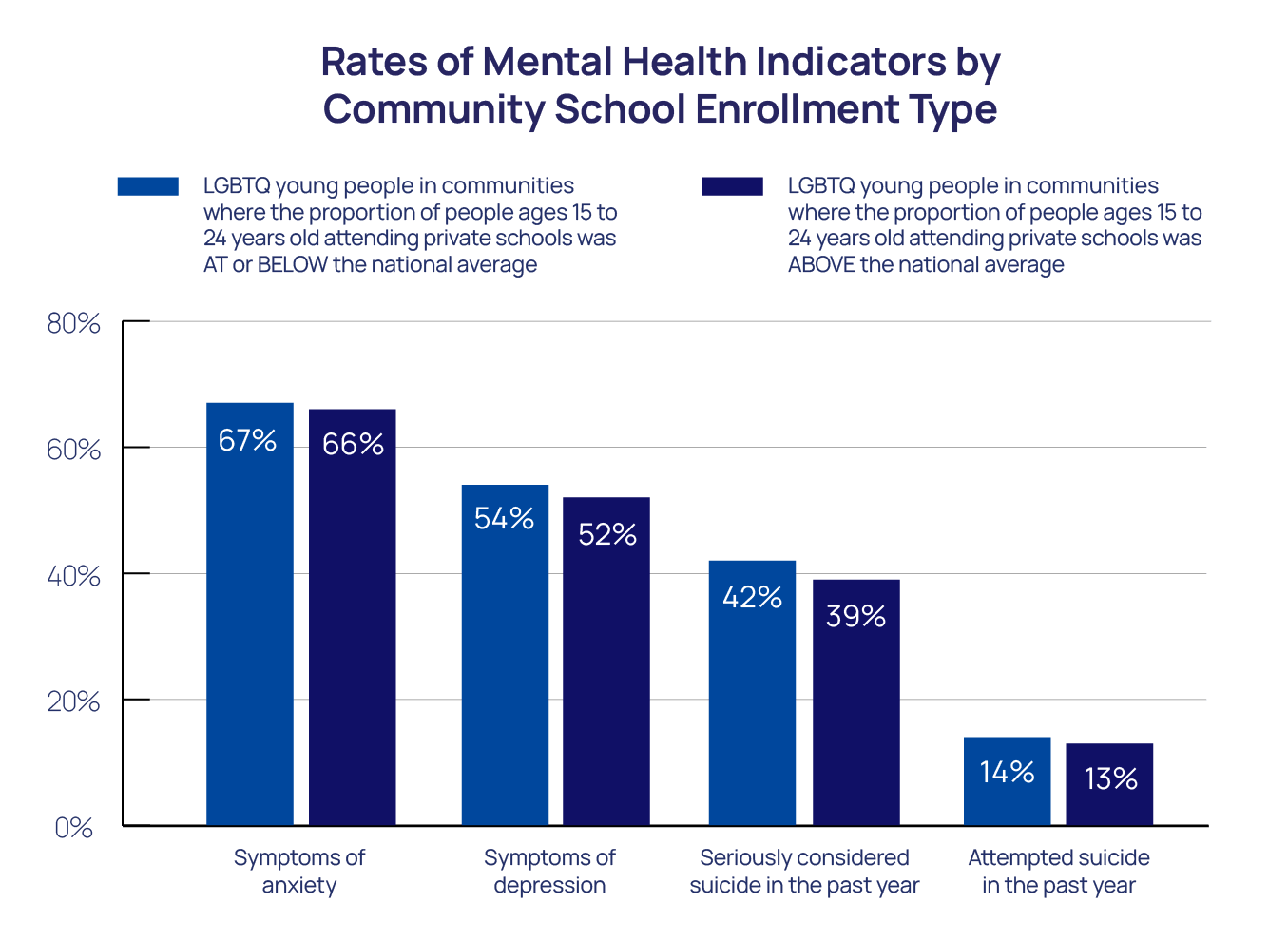
Overall, LGBTQ young people living in communities where the proportion of people ages 15 to 24 years old attending a private school was above the national average reported better mental health compared to LGBTQ young people living in communities where the proportion of people ages 15 to 24 years old attending private schools was at or below the national average. LGBTQ young people living in communities where the proportion of people ages 15 to 24 years old attending private schools was above the national average reported significantly lower rates of symptoms of anxiety (66% compared to 67%, p < 0.05), symptoms of depression (52% compared to 54%, p < 0.01), seriously considering suicide in the past year (39% compared to 42%, p < 0.01), and attempting suicide in the past year (13% compared to 14%, p < 0.05).
Community Military Service
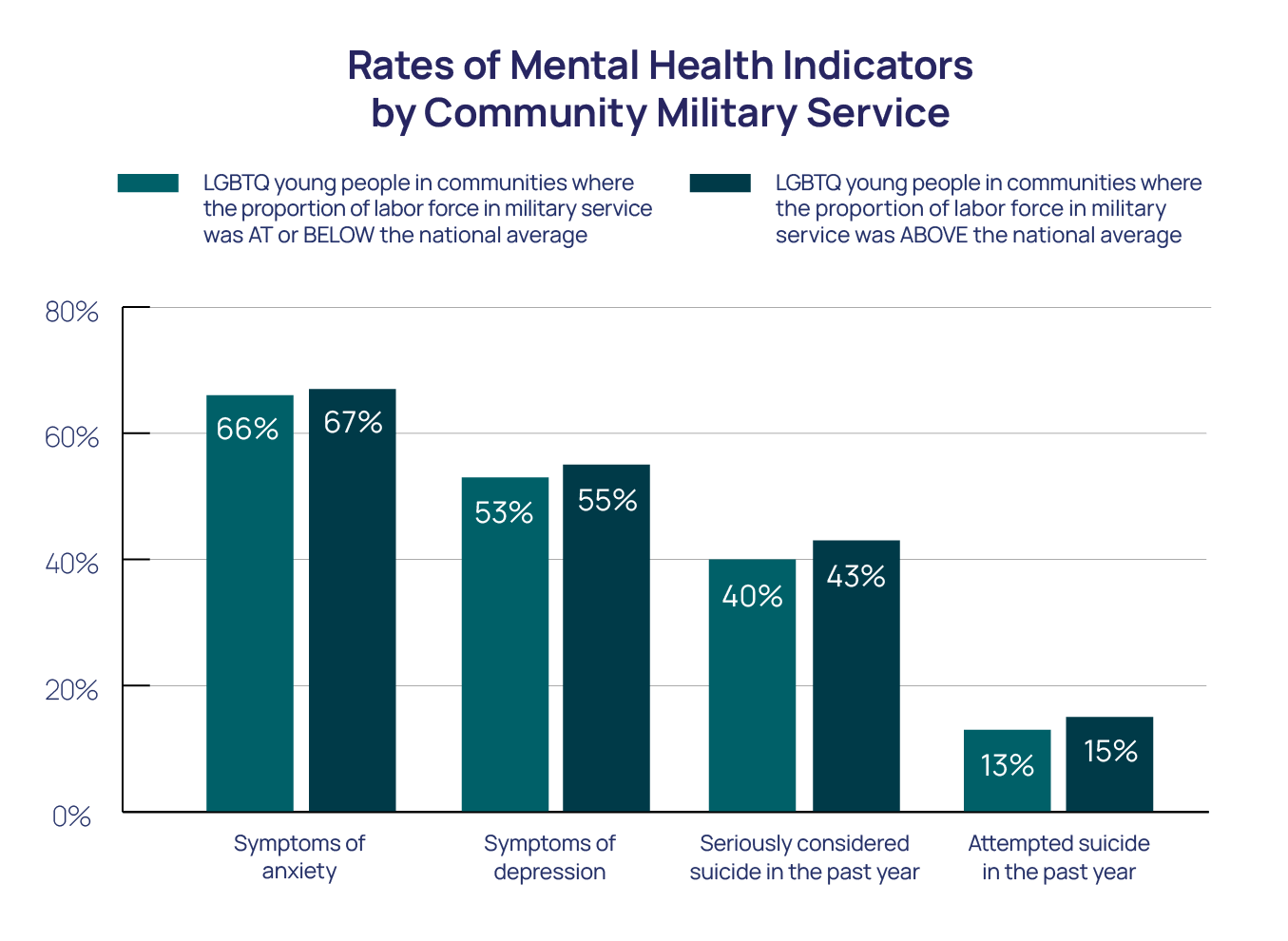
The proportion of the labor force in military service measures the level of military involvement of a community. Anti-LGBTQ attitudes originating from previously enforced anti-LGBTQ policies (such as “Don’t Ask, Don’t Tell” which was active between 1993 and 2011 [Feder, 2013], or the recently repealed ban on transgender military service) may remain in some communities with high community military service. There were no differences among LGBTQ young people across race, sexual orientation, or gender identity with regard to the proportion of the labor force in military service in the communities in which they live.
Overall, LGBTQ young people living in communities where the proportion of labor force in military service was at or below the national average reported better mental health outcomes compared to LGBTQ young people living in communities where the proportion of labor force in military service was above the national average. LGBTQ young people living in communities where the proportion of labor force in military service was at or below the national average reported lower rates of symptoms of depression (53% compared to 55%, p < 0.05), and seriously considering suicide in the past year (40% compared to 43%, p < 0.01). However, the rates of attempting suicide in the past year and symptoms of anxiety had no discernible differences among LGBTQ young people across communities related to the community military service.
RECOMMENDATIONS
Overall, these findings suggest that community-level environmental indicators are related to the mental health of LGBTQ young people. More specifically, factors such as living in less racial/ethnically diverse, lower-income, or less-populated communities, as well as areas with fewer same-sex couples or access to health insurance coverage, were all associated with poorer mental health among LGBTQ young people. In addition, individuals who identified as Native/Indigenous, Hispanic/Latinx, and Black were more likely to live in areas where a number of these indicators associated with poor mental health were present.
Stakeholders should dedicate additional resources to communities that are typically under-resourced in an effort to improve the mental health of LGBTQ young people. Lacking access to important preventative resources, such as health care and food/financial assistance programs, may underscore our findings at the community level. For example, the results revealed that in areas with less access to health insurance coverage, LGBTQ young people had higher rates of mental health concerns in comparison to areas with more health insurance coverage. Relatedly, LGBTQ young people in areas with lower income or fewer private schools had higher rates of mental health concerns. Benefits of having health insurance coverage and enough income to cover medical expenses can include improved management of current mental and physical health problems (e.g., medication adherence, treating chronic conditions), earlier detection and treatment of an illness, and improved psychological well-being due to being generally healthier and feeling confident about being able to access care when necessary (Sommers et al., 2017). Thus, the importance of providing access to affordable healthcare, as well as financial assistance programs for low-income families and young people, cannot be stressed enough. Offering equitable resources and affordable healthcare coverage, regardless of someone’s physical location, is an important step in helping LGBTQ young people prevent and address their mental health concerns.
Communities must create more affirming environments for LGBTQ young people. Given that being in a community with more same-sex couples in households was related to better mental health among LGBTQ young people, it is essential to consider ways of providing more LGBTQ-affirming environments and resources. Past research has identified that having an LGBTQ role model can have a positive impact on young people’s development and mental health (Bird et al., 2012). Being in an area with more visible same-sex couples may increase exposure to those role models and LGBTQ representation more broadly, possibly explaining these findings. It is also possible that these areas may feel safer for LGBTQ young people due to having more inclusive policies or resources, which can also impact mental health outcomes (Wight et al., 2013). It is likely that same-sex couples are more attracted to these areas as places to live for similar reasons. Relatedly, the creation of more LGBTQ-affirming spaces and community organizations may improve the mental health of LGBTQ young people through the identification of supportive friends and allies while engaging in community-building activities. People who seek to support LGBTQ young people can be welcoming to them and their friends/partners, be respectful and use affirming language, and remain educated about LGBTQ issues, which is reviewed in our 2022 National Survey. It is also essential to advocate for LGBTQ young people by supporting policies that protect the existence of LGBTQ affirming spaces and support LGBTQ young people in accessing LGBTQ-related educational information when needed. Lastly, actively listening and remaining informed about LGBTQ issues may also help LGBTQ young people feel safe, heard, and cared for in their communities.
Given that racially diverse communities appear to offer crucial mental health protection for all LGBTQ young people, racial diversity should be celebrated, and acceptance of others encouraged, in all communities. LGBTQ young people reported better mental health when they lived in communities that were more racially diverse or had more people who were born outside the U.S. For people of color, living in more racially diverse areas can be related to lower rates of racial discrimination (Dailey et al., 2010), which is often linked with more positive health outcomes (Kessler et al., 1999). For White LGBTQ young people, living in racially diverse communities may improve their mental health through a variety of avenues, such as through exposure to different perspectives (e.g., interacting with or learning about individuals outside of their own culture and background), the development of empathy towards others who have different life experiences, reducing social isolation, improving feelings of belonging, and being exposed to diverse role models. Communities are encouraged to embrace the diversity within one’s area, given its protective relationship with mental health.
Research should better explore how a young person’s community and environment relate to their mental health. Research often examines individual-level experiences; however, well-developed theory and previous research suggests that there are many levels of influence beyond individual experiences, including one’s community (Bronfenbrenner, 1992). LGBTQ young people frequently live with their parents and in the neighborhood that their parents chose for them. Similarly, many LGBTQ young people live in foster homes, group homes, or in another environment without their biological family, with even less choice about where they live or what resources they can access. Given the findings in this report, we know that community factors and caregivers’ access to resources may impact the mental health of LGBTQ young people. Researchers should continue to study ways to improve our communities in order for them to be more LGBTQ-affirming, so that LGBTQ young people can authentically express themselves in safe spaces, experience positive mental health, and be placed at lower risk of suicide, no matter where they live.
The Trevor Project is committed to working toward supporting LGBTQ young people and strengthening the communities in which they exist. Our counselors and staff are located in a variety of communities across the U.S., offering unique insights into those areas for intervention. For example, staff members often have a deeper understanding of their surrounding community, as well connections with local community organizations or government officials, which can assist with change efforts. Our advocacy team works to champion legislation that supports the mental health of LGBTQ young people at the national, state, and community level, including current efforts to ban conversion therapy throughout the U.S. In addition, our education department provides LGBTQ trainings in various communities, and TrevorSpace, our safe space social networking site, is available for LGBTQ young people ages 13 to 24, including those who may find themselves in less supportive environments. Lastly, our research team disseminates findings, including state-level reports, so that local community organizations can inform change efforts and receive proper support for the work they are doing to save young LGBTQ lives.
| The authors of this report acknowledge and extend our deepest thanks to Brooke A. Jarrett, PhD and Hannah R. Rosen for providing feedback and guidance on the creation of this report. |
About The Trevor Project
The Trevor Project is the leading suicide prevention and crisis intervention organization for LGBTQ young people. The Trevor Project offers a suite of 24/7 crisis intervention and suicide prevention programs, including TrevorLifeline, TrevorText, and TrevorChat, as well as the world’s largest safe space social networking site for LGBTQ young people, TrevorSpace. Trevor also operates an education program with resources for adults and organizations serving young people, an advocacy department fighting for pro-LGBTQ legislation and against anti-LGBTQ policies, and a research team to examine the most effective means to end suicide in LGBTQ young people. If you or someone you know is feeling hopeless or suicidal, our trained crisis counselors are available 24/7 at 1-866-488-7386, via chat TheTrevorProject.org/Help, or by texting 678-678.
This report is a collaborative effort from the following individuals at The Trevor Project:
Wilson Y. Lee, MS
Senior Machine Learning Research Scientist
Jonah P. DeChants, PhD
Senior Research Scientist
Myeshia N. Price, PhD
Director of Research Science
Carrie K. Davis, MSW
Chief Community Officer
J. Nicholas Hobbs, MS
Senior Machine Learning Research Scientist
Steven Hobaica, PhD
Research Scientist
Ronita Nath, PhD
Vice President of Research
Recommended Citation: Lee, W. Y., Hobbs, J. N., DeChants, J. P., Hobaica, S., Price, M. N., Nath, R., & Davis, C. K. (2023). The association of community-level environmental indicators on the mental health of LGBTQ young people. The Trevor Project.
Media inquiries:
[email protected]
Research-related inquiries:
[email protected]
REFERENCES
- American Hospital Association. (2022). The importance of health coverage. October, 2019.
- Baams, L., Grossman, A. H., & Russell, S. T. (2015). Minority stress and mechanisms of risk for depression and suicidal ideation among lesbian, gay, and bisexual youth.Developmental Psychology, 51(5), 688–696. https://doi.org/10.1037/a0038994
- Bai, X., Ramos, M. R., & Fiske, S. T. (2020). As diversity increases, people paradoxically perceive social groups as more similar. Proceedings of the National Academy of Sciences, 117(23), 12741-12749.
- Bird, J. D., Kuhns, L., & Garofalo, R. (2012). The impact of role models on health outcomes for lesbian, gay, bisexual, and transgender youth. Journal of Adolescent Health, 50(4), 353–357. https://doi.org/10.1016/j.jadohealth.2011.08.006
- Bronfenbrenner, U. (1992). Ecological systems theory. Jessica Kingsley Publishers.
- Badgett, M. V. L., Carpenter, C. S., & Sansone, D. (2021). LGBTQ economics. Journal ofEconomic Perspectives, 35(2), 141–170. https://doi.org/10.1257/jep.35.2.141
- Dailey, A. B., Kasl, S. V., Holford, T. R., Lewis, T. T., & Jones, B. A. (2010). Neighborhood-and individual-level socioeconomic variation in perceptions of racial discrimination. Ethnicity & Health, 15(2), 145–163. https://doi.org/10.1080/13557851003592561
- Duncan, D. T., & Hatzenbuehler, M. L. (2014). Lesbian, gay, bisexual, and transgender hate crimes and suicidality among a population-based sample of sexualminority adolescents in Boston. American Journal of Public Health, 104(2), 272–278. https://doi.org/10.2105/AJPH.2013.301424
- Durso, L. E. (2018). Progress and challenges in sexual orientation and gender identity measurement in the first Year of the Trump administration. American Journal of Public Health, 108(7), 894–895. https://doi.org/10.2105/AJPH.2018.304476
- Ellis, A.R., Konrad, T.R., Thomas, K.C., & Morrissey, J.P. (2009). County-Level Estimates of Mental Health Professional Supply in the United States. Psychiatric Services, 60(10), 1314–1322. https://doi.org/10.1176/ps.2009.60.10.1315
- Feder, J. (2013). “Don’t Ask, Don’t Tell”: A Legal Analysis.
- Flaskerud, J. H., & Lesser, J. (2018). The current socio-political climate and psychological distress among transgender people. Issues in Mental Health Nursing, 39(1), 93–96. https://doi.org/10.1080/01612840.2017.1368751
- Gates, G. J. (2013). Same-sex and different-sex couples in the American Community Survey: 2005-201. The Williams Institute. https://escholarship.org/content/qt8dk71277/qt8dk71277.pdf
- Hatzenbuehler, M. L. (2011). The social environment and suicide attempts in lesbian, gay, and bisexual youth. Pediatrics, 127(5), 896–903. https://doi.org/10.1542/peds.2010-3020
- Hatzenbuehler, M. L., & Keyes, K. M. (2013). Inclusive anti-bullying policies and reduced risk of suicide attempts in lesbian and gay youth. Journal of Adolescent Health, 53(1), S21–S26. https://doi.org/10.1016/j.jadohealth.2012.08.010
- Hill, R. M., & Pettit, J. W. (2012). Suicidal ideation and sexual orientation in college students: The roles of perceived burdensomeness, thwarted belongingness, and perceived rejection due to sexual orientation. Suicide and Life-Threatening Behavior, 42(5), 567–579. http://dx.doi.org/10.1111/j.1943-278X.2012.00113.x
- Jepsen, C., & Jepsen, L. (2022). Convergence over time or not? U.S. wages by sexual orientation, 2000–2019. Labour Economics, 74, 102086. https://doi.org/10.1016/j.labeco.2021.102086
- Johns, M. M., Lowry, R., Andrzejewski, J., Barrios, L. C., Demissie, Z., McManus, T., Rasberry, C. N., Robin, L., & Underwood, J. M. (2019). Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school students—19 states and large urban school districts, 2017. MMWR Morbidity and Mortality Weekly Report, 68(3), 67–71. https://doi.org/10.15585/mmwr.mm6803a3
- Johns, M. M., Lowry, R., Haderxhanaj, L. T., Rasberry, C. N., Robin, L., Scales, L., Stone, D., & Suarez, N. A. (2020). Trends in violence victimization and suicide risk by sexual identity among high school students—youth risk behavior survey, United States, 2015–2019. MMWR Morbidity Mortality Weekly Report, 69(Suppl-1), 19–27. https://doi.org/10.15585/mmwr.su6901a3
- Kessler, R. C., Mickelson, K. D., & Williams, D. R. (1999). The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. Journal of Health and Social Behavior, 40(3), 208–230. https://doi.org/10.2307/2676349
- Kingsbury, M., Clayborne, Z., Colman, I., & Kirkbride, J. B. (2020). The protective effect of neighbourhood social cohesion on adolescent mental health following stressful life events. Psychological Medicine, 50(8), 1292–1299. https://doi.org/10.1017/S0033291719001235
- Kosciw, J. G., Greytak, E. A., Zongrone, A. D., Clark, C. M., & Truong, N. L. (2018). The 2017 national school climate survey: The experiences of lesbian, gay, bisexual, transgender, and queer youth in our nation’s schools. GLSEN. https://www.glsen.org/sites/default/files/2019-10/GLSEN-2017-National-School-Climate-Survey-NSCS-Full-Report.pdf
- Lau, A. S., Tsai, W., Shih, J., Liu, L. L., Hwang, W. C., & Takeuchi, D. T. (2013). The immigrant paradox among Asian American women: Are disparities in the burden of depression and anxiety paradoxical or explicable? Journal of Consulting and Clinical Psychology, 81(5), 901–911. https://doi.org/10.1037/a0032105
- Manson, S. M., Schroeder, J., Van Riper, D., Kugle, T., & Ruggles, S. (2022). IPUMS national historical geographic information system: version 17.0. http://doi.org/10.18128/D050.V17.0
- Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. https://doi.org/10.1037/0033-2909.129.5.674
- Plummer, F., Manea, L., Trepel, D., & McMillan, D. (2016). Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. General Hospital Psychiatry, 39, 24–31. https://doi.org/10.1016/j.genhosppsych.2015.11.005
- Pollitt, A. M., Ioverno, S., Russell, S. T., Li, G., & Grossman, A. H. (2021). Predictors and mental health benefits of chosen name use among transgender youth. Youth & Society, 53(2), 320–341. https://doi.org/10.1177/0044118X19855898
- Price-Feeney, M., Green, A. E., & Dorison, S. (2020). Understanding the mental health of transgender and nonbinary youth. Journal of Adolescent Health, 66(6), 684–690. https://doi.org/10.1016/j.jadohealth.2019.11.314
- Reidenberg, D., & Berman, A. L. (2017). Changing the direction of suicide prevention in the United States. Suicide and Life-Threatening Behavior, 47(4), 509–517. https://doi.org/10.1111/sltb.12310
- Richardson, L. P., Rockhill, C., Russo, J. E., Grossman, D. C., Richards, J., McCarty, C., McCauley, E., & Katon, W. (2010). Evaluation of the PHQ-2 as a brief screen for detecting major depression among adolescents. Pediatrics, 125(5), e1097-e1103. https://doi.org/10.1542/peds.2009-2712
- Russell, S. T., & Fish, J. N. (2016). Mental health in lesbian, gay, bisexual, and transgender (LGBT) youth. Annual Review of Clinical Psychology, 12(1), 465–487. https://doi.org/10.1146/annurev-clinpsy-021815-093153
- Ryan, C., Huebner, D., Diaz, R. M., & Sanches, J. (2009). Family rejection as a predictor of negative health outcomes in white and Latino lesbian, gay, and bisexual young adults. Pediatrics, 123(1), 346–352. https://doi.org/10.1542/peds.2007-3524
- Sommers, B. D., Gawande, A. A., & Baicker, K. (2017). Health insurance coverage and health—what the recent evidence tells us. New England Journal of Medicine, 377(6), 586–593.
- The Trevor Project. (2023). 2023 U.S. national survey on the mental health of LGBTQ young people. https://www.thetrevorproject.org/survey-2023/
- Tudge, J. R. H., Merçon-Vargas, E. A., & Payir, A. (2022). Urie Bronfenbrenner’s Bioecological Theory: Its Development, Core Concepts, and Critical Issues. In K. Adamsons, A. L. Few-Demo, C. Proulx, & K. Roy (Eds.), Sourcebook of Family Theories and Methodologies (pp. 235–254). Springer International Publishing. https://doi.org/10.1007/978-3-030-92002-9_16
- U.S. Census Bureau. (2017). American Community Survey information guide. https://www.census.gov/content/dam/Census/programs-surveys/acs/about/ACS_Information_Guide.pdf
- U.S. Census Bureau. (2022). U.S. Census Bureau’s budget fiscal year 2023. U.S. Department of Commerce. https://www.commerce.gov/sites/default/files/2022-03/FY2023-Census-Congressional-Budget-Submission.pdf
- Velez, B. L., Zelaya, D., & Scheer, J. (2021). Context Matters: Minority Stress and Mental Health Experiences of Diverse LGBTQ People. In K. L. Nadal & M. R. Scharrón-del Río (Eds.), Queer Psychology (pp. 103–117). Springer International Publishing. https://doi.org/10.1007/978-3-030-74146-4_6
- Wight, R. G., LeBlanc, A. J., & Lee Badgett, M. V. (2013). Same-sex legal marriage and psychological well-being: Findings from the California Health Interview Survey. American Journal of Public Health, 103(2), 339–346. https://doi.org/10.2105/AJPH.2012.301113
- Yeung, W. J., & Conley, D. (2008). Black–white achievement gap and family wealth. Child Development, 79(2), 303-324. https://doi.org/10.1111/j.1467-8624.2007.01127.x
© The Trevor Project 2023