Youth's Lives Every Day
Key Findings
Compared to LGBTQ+ young people living in non-rural areas, those in rural areas:
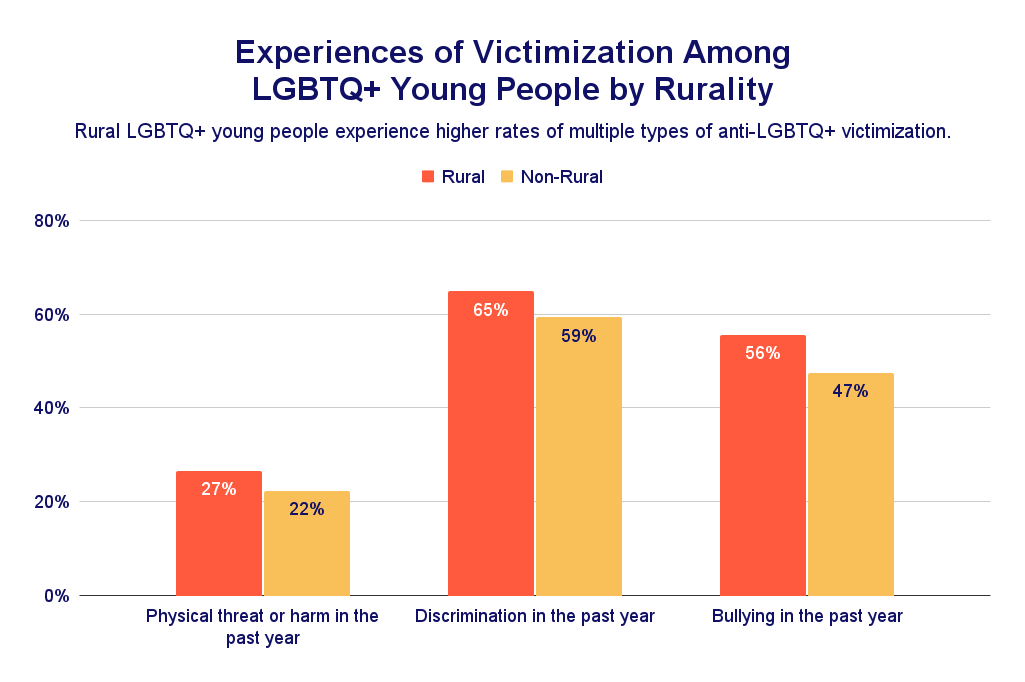
- Face higher rates of victimization, including physical threats or harm (27% vs. 22%) and bullying (56% vs. 47%).
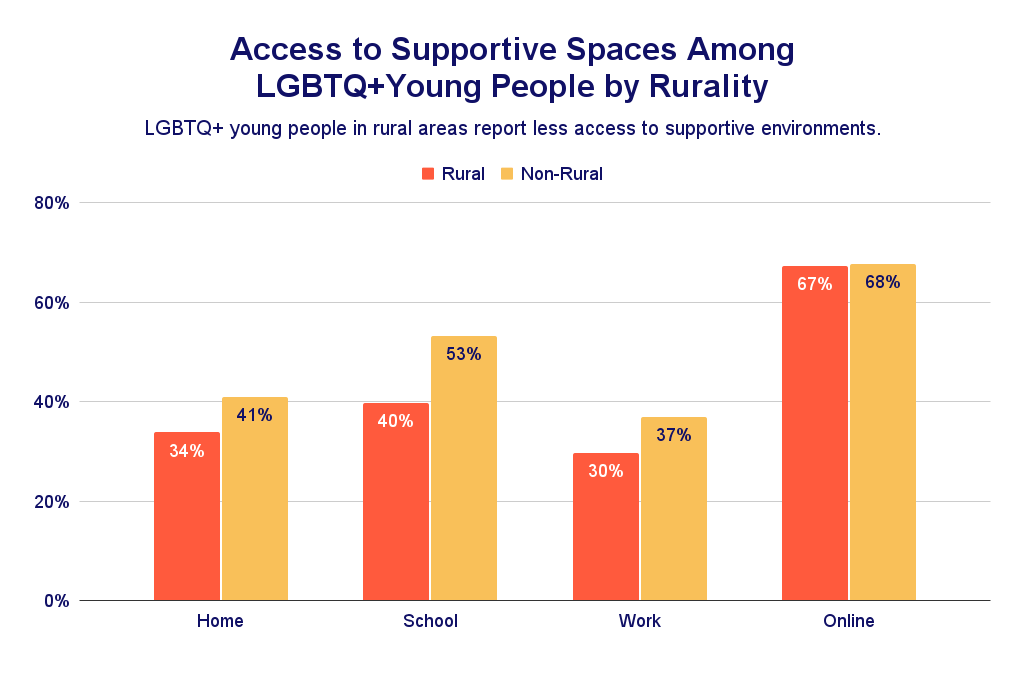
- Report fewer supportive spaces, including at home (34% vs. 41%) and school (40% vs. 53%).
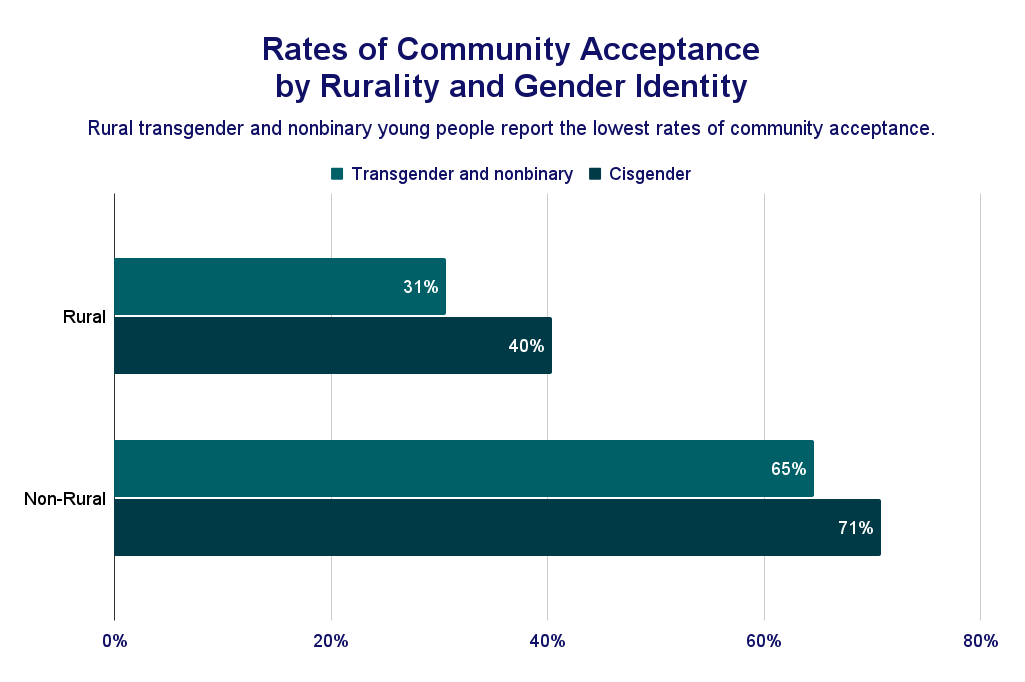
- Are half as likely to say their community is supportive (34% vs. 67%), with TGNB young people reporting even lower rates (31% TGNB vs. 40% cisgender rural youth).
- Are more likely to have considered suicide (43% vs. 38%).
- Have less access to mental health care, with only 47% of those who wanted care able to get it, compared to 51% in non-rural areas.
Background
Geographic location is associated with several determinants of health, such as housing, air and water quality, access to education and employment, and the availability of health care — to the extent that life expectancy can differ by nearly nine years depending on the state in which a person lives.1,2 Location can further influence health due to its association with policy and the social environment, which are two relevant factors for the well-being of LGBTQ+ young people. Despite the robust link between location and health, there remains sparse research on how rural environments shape the health of people who live there.3 There is growing research about the relationship between rurality and the health of LGBTQ+ people, although most of this work features data from cisgender lesbian, gay, and bisexual adults.4 Using data from The Trevor Project’s 2024 U.S. National Survey on the Mental Health of LGBTQ+ Young People, this brief seeks to contribute to the knowledge base of what is known about the experiences of LGBTQ+ young people living in rural areas by documenting differences across a variety of health and wellness indicators.
Results
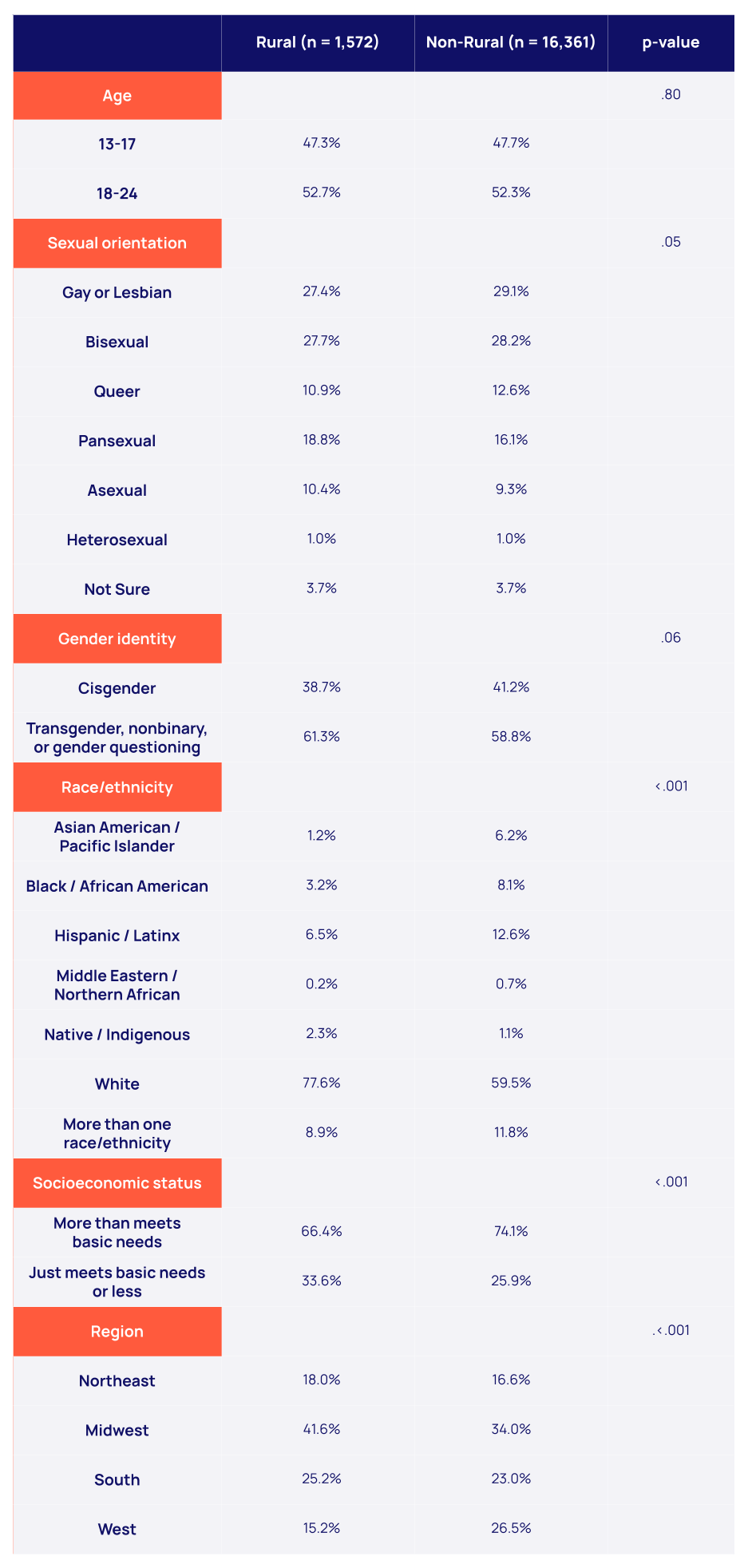
A minority (9%) of LGBTQ+ young people reported living in a rural area, with the rest living in a large city (18%), suburb (36%), or a small town (38%). While rural and non-rural LGBTQ+ young people shared many demographic similarities, rural respondents were less likely to be people of color than non-rural respondents (22% vs. 41%). Rural residents were also more likely to report that they were just able to meet their basic needs, if at all, compared to non-rural residents (34% vs. 26%).
Compared to LGBTQ+ young people living in non-rural areas, those in rural areas were more likely to report experiences of physical threat or harm (27% vs. 22%) and discrimination (65% vs. 60%) due to their sexual orientation or gender identity in the past year. Rural respondents were also more likely to report a past-year experience of in-person or online bullying compared to their non-rural counterparts (56% vs. 47%). Additionally, there were differences in access to supportive spaces, with rural respondents being less likely to report that their home (34% vs. 41%), school (40% vs. 53%), and work (30% vs. 37%) environments were supportive of their LGBTQ+ identity compared to non-rural respondents. However, support in online spaces did not differ between rural and non-rural LGBTQ+ young people, with 68% of all respondents reporting access to an online space that was supportive of their LGBTQ+ identity.
The majority (67%) of non-rural LGBTQ+ young people said the community where they live was supportive of LGBTQ+ people, though only 34% of rural respondents said the same. Notably, this difference was even more pronounced by gender identity. Among rural residents, 40% of those who were cisgender said their community was supportive, while only 31% of rural transgender and nonbinary young people reported that their community was supportive.
For LGBTQ+ young people, living in a rural area was associated with greater difficulty accessing mental health care, worse mental health outcomes, and higher rates of suicidal thoughts and behaviors compared to their non-rural peers. In particular, LGBTQ+ young people living in rural areas were more likely to report recent symptoms of anxiety (71% vs. 65%) and depression (58% vs. 52%). They were also more likely than non-rural residents to have considered suicide in the past-year (43% vs. 38%), although there was no statistically significant difference in suicide attempts. Additionally, LGBTQ+ young people living in rural areas had less access to mental health care, with only 47% of those who wanted mental health care able to get it compared to 51% of their non-rural counterparts. Among those who were able to access mental health care, rural residents were more likely than non-rural residents to report receiving individual therapy in-person (74% vs. 68%) and less likely to receive therapy online (46% vs. 54%).
Recognizing that these differences may be attributable to demographic variations, we controlled for race/ethnicity, gender identity, sexual orientation, socioeconomic status, region, and age. The effect of rurality persisted across most outcomes (using in-person therapy was no longer statistically significant), indicating that the effect of living in a rural area for LGBTQ+ young people is both robust and distinct.
Looking Ahead
For LGBTQ+ young people, rurality is associated with a variety of health indicators and experiences, even after adjusting for several demographic factors. Compared to non-rural LGBTQ+ young people, rural respondents reported greater likelihood of victimization, discrimination, and bullying, less access to supportive spaces, and lower rates of receiving desired mental health care. They also reported being more likely to have recent symptoms of anxiety, depression, and having considered suicide in the past year. These findings highlight the need to both target and design resources specifically for LGBTQ+ young people living in rural areas.
Consistent with national trends, LGBTQ+ young people living in rural areas were less likely to be able to access desired mental health care than those in non-rural areas.5 Unexpectedly, however, was that among those who were able to access mental health care, they were less likely than non-rural respondents to utilize online therapy. The Internet is often considered as a way to extend access to areas with relatively fewer health care resources, and its promise in less densely populated rural areas is frequently touted. Our findings are consistent with other research that suggests that while interest in these technologies may be high, there remains a lot of work to make them accessible to rural residents.6 An encouraging finding, however, is that rural LGBTQ+ young people were just as likely as non-rural LGBTQ+ young people to have access to a supportive online environment. With sufficient resources, mental health care providers may be well-positioned to provide much-needed online services to LGBTQ+ young people in rural areas.
There are well-documented challenges in engaging residents of rural areas to participate in both public health research and intervention.7,8 Unfortunately, these challenges may be exacerbated for LGBTQ+ young people, whether it be via their ability to access research opportunities or concerns about disclosing their LGBTQ+ status. Our own research is not immune to these challenges; despite approximately 20% of the U.S. population living in a rural area, less than 10% of our survey participants reported the same. Though we adjusted our analyses for census region, we know little about how the experiences of LGBTQ+ young people vary across different rural contexts. Rural environments are incredibly diverse; the experiences of LGBTQ+ young people in the South are likely very different from those in Appalachia or the Northwest.9
When we asked LGBTQ+ young people about the community where they live, those in rural areas were twice as likely to say that it was not accepting of LGBTQ+ people. This finding was particularly pronounced for transgender and nonbinary people: less than one-third said their community was accepting. In many ways this may be the most important metric – until LGBTQ+ young people in rural areas feel welcomed and supported in their own communities, health inequities will persist. These findings offer a broad picture of several challenges faced by LGBTQ+ young people in rural areas. We hope they can catalyze additional research to support rural LGBTQ+ populations.
The Trevor Project is committed to supporting LGBTQ+ young people through crisis intervention, research, and advocacy initiatives. TrevorSpace, our dedicated social media platform, offers LGBTQ+ young people a safe and supportive community where they can connect with supportive peers, regardless of where they live. Our 24/7 crisis services—available by phone, chat, and text—ensure that LGBTQ+ young people have access to highly trained counselors whenever they need help. Our education team empowers adults with the tools and knowledge to effectively support LGBTQ+ young people across all identities, while our advocacy team works to promote access to welcoming environments in all geographic areas, both at the federal and state level. Additionally, we are committed to continuing to publish research focused on the relationship between rurality and LGBTQ+ mental health.
You can read more related research from The Trevor Project here: The Association of Community Level Environmental Indicators on the Mental Health of LGBTQ+ Young People and LGBTQ Youth in Small Towns and Rural Areas. Anti-LGBTQ+ School Policies and LGBTQ+ Young People and State-Level Anti-Transgender Laws Increase Past-Year Suicide Attempts among Transgender and Non-Binary Young People. Additionally, The Trevor Project provides resources for both LGBTQ+ young people and their allies, such as How to Signal You are an Ally in a Hostile Environment.
Data Tables
Demographic Characteristics of LGBTQ+ Young People Living in Rural and Non-Rural Areas
Rural LGBTQ+ Young People’s Experiences Compared to Non-Rural LGBTQ+ Young People

Logistic regression models controlled for age, sexual orientation, gender identity, race/ethnicity, socioeconomic status, and region.
Methods
References
Recommended Citation
The Trevor Project. (2025). The Mental Health and Experiences of LGBTQ+ Young People in the Rural U.S. https://doi.org/10.70226/XAGT4119
For more information please contact: [email protected]
© The Trevor Project 2025